🧠 Cerebral Blood Supply
Inflow, outflow, and the clinical danger zones — a complete anatomical and clinical study guide.
Cerebral Blood Supply — The Inflow
The brain receives its blood supply from two paired arterial systems that ultimately unite at the base of the brain: the Internal Carotid Arteries (anterior circulation) and the Vertebral Arteries (posterior circulation). Together they form the Circle of Willis, the brain’s vital safety net.
Origin & Path
The ICA arises from the bifurcation of the common carotid artery at the level of the upper border of the thyroid cartilage (C4). It ascends through the neck without giving off any branches — this is the “golden rule” that distinguishes it from the external carotid artery, which gives off multiple branches in the neck.
The Golden Rule — ICA Has NO Neck Branches
In neck dissections and carotid endarterectomies, the key rule is: the ICA is branchless in the neck. Any artery giving off branches in the neck is the External Carotid Artery (ECA). This distinction is critical when surgically exposing the carotid bifurcation.
Skull Entry & Cavernous Course
The ICA enters the skull base through the Carotid Canal in the petrous temporal bone. It does not pass through the Foramen Lacerum — it passes horizontally over it, since the foramen is plugged with fibrocartilage in life.
It then takes a tortuous S-shaped path called the “carotid siphon” directly through the blood-filled lumen of the Cavernous Sinus. Here it is surrounded by a post-ganglionic sympathetic plexus and runs immediately adjacent to the Abducens nerve (CN VI) — which is why CN VI is the first nerve affected in cavernous pathology.
Intracranial Branches — OPCAM
Once the ICA enters the intracranial space, it gives off five major cerebral branches. Remember them with:
Ophthalmic Artery
First major intracranial branch. Enters the orbit via the optic canal. Occlusion → sudden painless monocular blindness (amaurosis fugax).
Posterior Communicating Artery (PComm)
Connects the ICA to the posterior cerebral artery — part of the Circle of Willis. A PComm aneurysm classically compresses CN III, causing a painful, “surgical” pupil-involving third nerve palsy.
Anterior Choroidal Artery
Supplies the posterior limb of the internal capsule, choroid plexus, hippocampus, and amygdala. Small vessel, but a stroke here causes devastating contralateral hemiplegia, hemisensory loss, and hemianopia.
Anterior Cerebral Artery (ACA)
Supplies the medial surface of the frontal and parietal lobes. Occlusion causes contralateral leg weakness (leg area is on the medial cortex). Both ACAs are connected by the anterior communicating artery.
Middle Cerebral Artery (MCA)
The largest and most clinically important branch. Supplies the lateral surface of the frontal, parietal, and temporal lobes — including Broca’s area (speech production) and the arm/face motor cortex. The most common site of ischaemic stroke.
Origin & Path
The vertebral artery is the first and largest branch of the subclavian artery. It ascends through the transverse foramina (foramina transversaria) of vertebrae C6 to C1 — notably it skips C7. At C1 it grooves the posterior arch of the atlas in the suboccipital triangle, then pierces the dura and enters the skull via the Foramen Magnum.
Subclavian Branches — “VIT C & D”
Remember the branches of the subclavian artery with VIT C & D:
Vertebral | Internal Thoracic | Thyrocervical trunk | Costocervical trunk | Dorsal Scapular
Termination — The Basilar Artery
At the caudal border of the pons, the two vertebral arteries unite to form the single Basilar Artery. The vertebrobasilar system supplies the brainstem, cerebellum, and the posterior cerebral hemispheres (occipital lobes). Vertebrobasilar ischaemia is suggested by the “5 Ds”: Diplopia, Dysarthria, Dysphagia, Dizziness, and Drop attacks.
Vertebral Artery Branches
Posterior inferior cerebellar artery (PICA) — supplies the lateral medulla and inferior cerebellum. PICA occlusion → Lateral Medullary (Wallenberg) Syndrome.
Basilar Artery Branches
Anterior inferior cerebellar artery (AICA), pontine perforators, superior cerebellar artery (SCA). Basilar artery occlusion is catastrophic — “locked-in syndrome.”
Terminal Branches
The basilar artery terminates by bifurcating into the two Posterior Cerebral Arteries (PCAs), which supply the occipital lobes. PCA occlusion → contralateral homonymous hemianopia with macular sparing.
Anatomy & Function
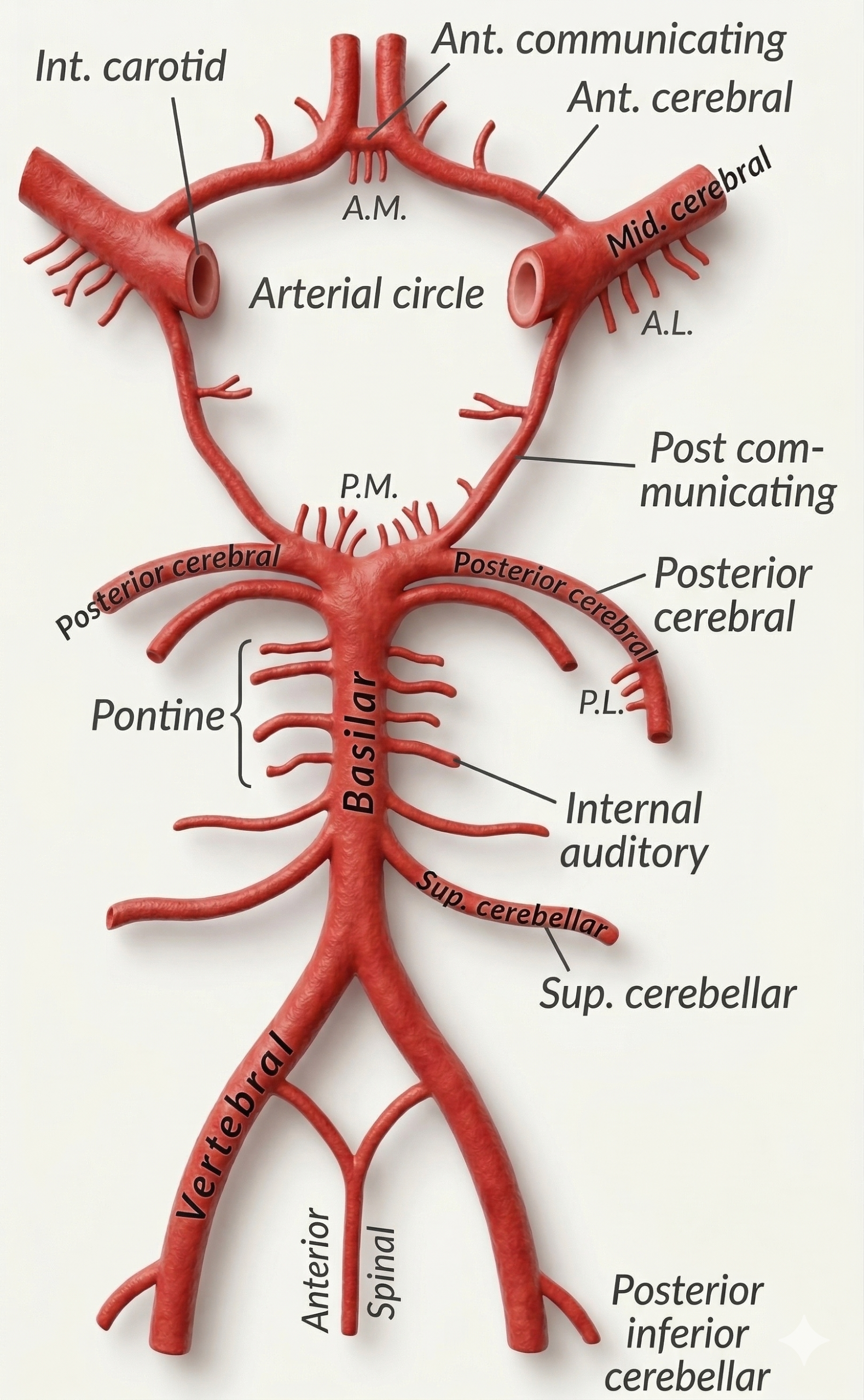
The Circle of Willis at the top, with the vertebral and common carotid arteries supplying it. The right side shows subclavian stenosis causing ‘subclavian steal’ — blood is retrograde drawn from the vertebral artery.
The Circle of Willis is a vital arterial anastomosis at the base of the brain that connects the anterior (ICA) and posterior (vertebrobasilar) circulations. Its purpose is to provide collateral blood flow — if one major vessel is occluded, blood can re-route around the circle to maintain perfusion. However, in practice only ~25% of people have a complete, well-formed Circle of Willis.
| Component | Origin | Role in the Circle |
|---|---|---|
| Anterior Communicating Artery (AComm) | Connects left and right ACA | Most common site for Berry aneurysms and SAH |
| Anterior Cerebral Arteries (ACA × 2) | ICA terminal branch | Anterior limbs of the circle |
| Internal Carotid Arteries (ICA × 2) | Common carotid bifurcation | Lateral connections to the circle |
| Posterior Communicating Arteries (PComm × 2) | ICA → PCA | Connect anterior and posterior circulations; aneurysm here causes CN III palsy |
| Posterior Cerebral Arteries (PCA × 2) | Basilar artery terminus | Posterior limbs; supply occipital lobes |
Berry Aneurysms & Subarachnoid Haemorrhage (SAH)
The Circle of Willis is the most common site for Berry (saccular) aneurysms. These arise at arterial junctions where the tunica media (muscular wall) is congenitally weakest — like a blowout at the weakest point of a tyre.
Classic Presentation of SAH — “Thunderclap Headache”
A ruptured Berry aneurysm causes a sudden, instantaneous, maximal headache — described as a “thunderclap” or “hammer blow to the back of the head.” The patient often reports it as “the worst headache of my life.” Associated features include nausea, photophobia, neck stiffness (meningism), and loss of consciousness. CT head without contrast will show blood filling the basal cisterns in a characteristic “star” sign. If CT is negative within 6 hours, a lumbar puncture should be performed looking for xanthochromia.
| Aneurysm Site | Frequency | Key Clinical Feature |
|---|---|---|
| Anterior Communicating Artery | Most common (~35%) | SAH; can compress optic chiasm → bitemporal hemianopia |
| Posterior Communicating Artery | Common (~30%) | Compresses CN III → painful pupil-involving third nerve palsy (“down and out” eye, blown pupil) |
| Middle Cerebral Artery bifurcation | Common (~20%) | SAH ± intracerebral haemorrhage; large haematoma may cause mass effect |
| Basilar Tip | Less common (~10%) | SAH; can compress CN III bilaterally |