🟠 The Pancreas
Complete MRCS revision covering anatomy, acute & chronic pancreatitis, pancreatic cancer, endocrine tumours, cystic lesions, the Whipple’s procedure, and clinical pearls.
Pancreatic Anatomy
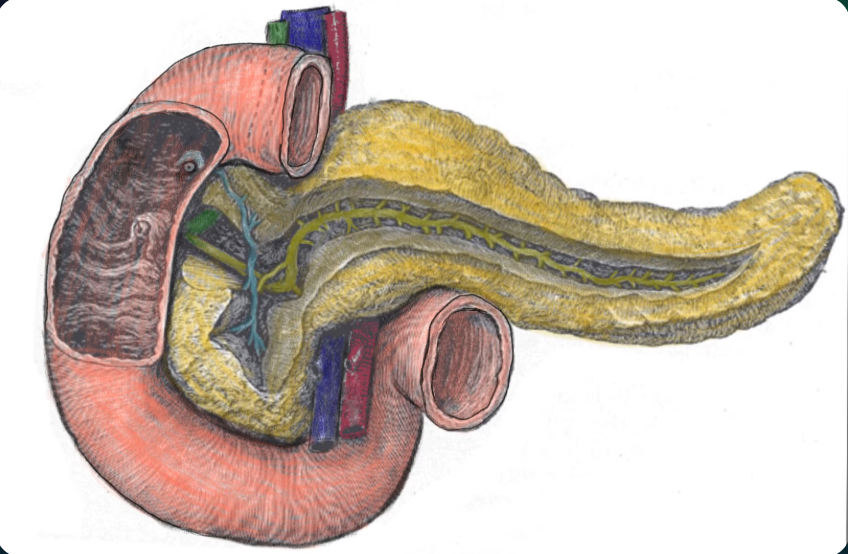
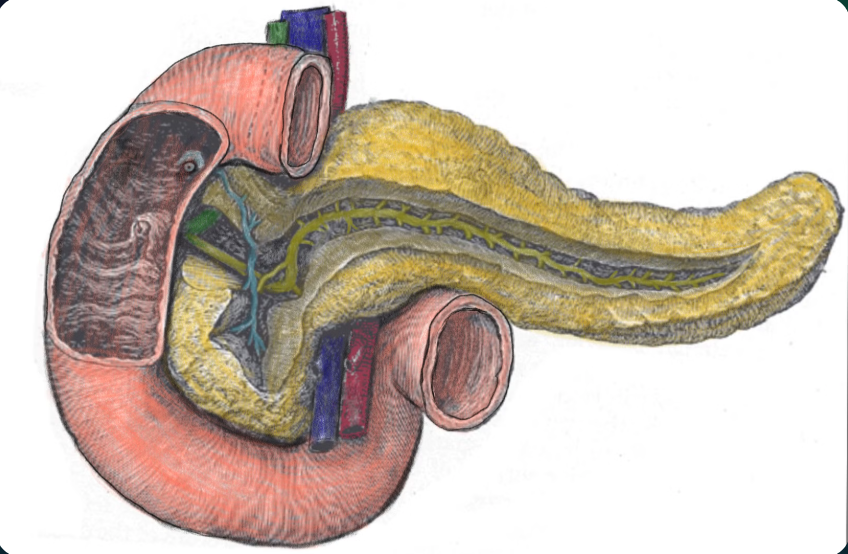
Hand drawing of the pancreas, duodenum and portal triad
The pancreas is an elongated, oblong-shaped accessory digestive gland with both endocrine and exocrine functions. It lies retroperitoneally (except for the tail, which is intraperitoneal) across the posterior abdominal wall at the level of the transpyloric plane (L1).
| Function | Cells / Structure | Products |
|---|---|---|
| Exocrine (85%) | Acinar cells → small ducts → main duct (Wirsung) → ampulla of Vater | Proteases (trypsin, chymotrypsin, carboxypeptidase), lipases (lipase, phospholipase, esterase), glycolytic enzymes (amylase, lactase), nucleolytic enzymes (RNase, DNase) + bicarbonate-rich fluid from ductal cells |
| Endocrine | Islets of Langerhans (α, β, δ, PP cells) | Insulin (β), Glucagon (α), Somatostatin (δ), Pancreatic polypeptide (PP), Ghrelin, Amylin, C-peptide |
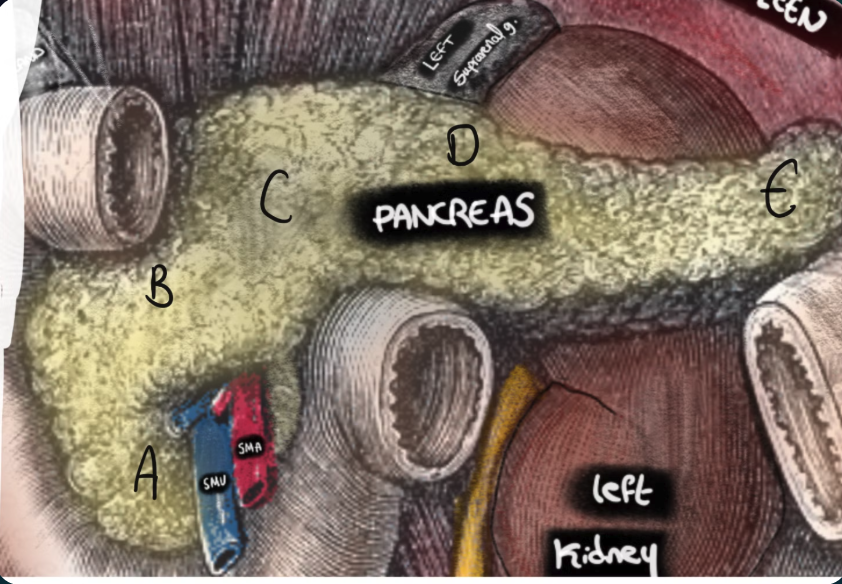
Diagram showing pancreas divisions labelled A–E
-
A
Uncinate Process
- Projects inferiorly from the pancreatic head
- Sits posterior to the superior mesenteric vessels (SMA and SMV pass over it) — key for Whipple’s
- Embryologically derived from the ventral pancreatic bud
-
B
Head of Pancreas
- Widest part — sits in the C-shaped groove of the duodenum (D1 anterior, D2 lateral, D3 inferior)
- Separate blood supply from the rest of the pancreas
- Contains the common bile duct (variable — partially covered in ~50%, fully embedded in ~30%)
- Removed in a Whipple’s procedure
-
C
Neck of Pancreas
- Sits anterior to the superior mesenteric vessels — the SMA and SMV run directly behind the neck. Portal vein forms here (SMV + splenic vein union).
- Critical plane for pancreatic transection in Whipple’s — the “retropancreatic tunnel” is developed anterior to SMV here
-
D
Body of Pancreas
- Continues from the neck, crossing the vertebral column
- Lies anterior to the splenic vein (which runs in the groove along the posterior surface)
- Anterior to the aorta at L2, left adrenal gland, and left kidney
-
E
Tail of Pancreas
- The only intraperitoneal part — connected to the spleen via the lienorenal (splenorenal) ligament
- Closely related to the splenic hilum and left colic flexure
- Risk of splenectomy during distal pancreatectomy
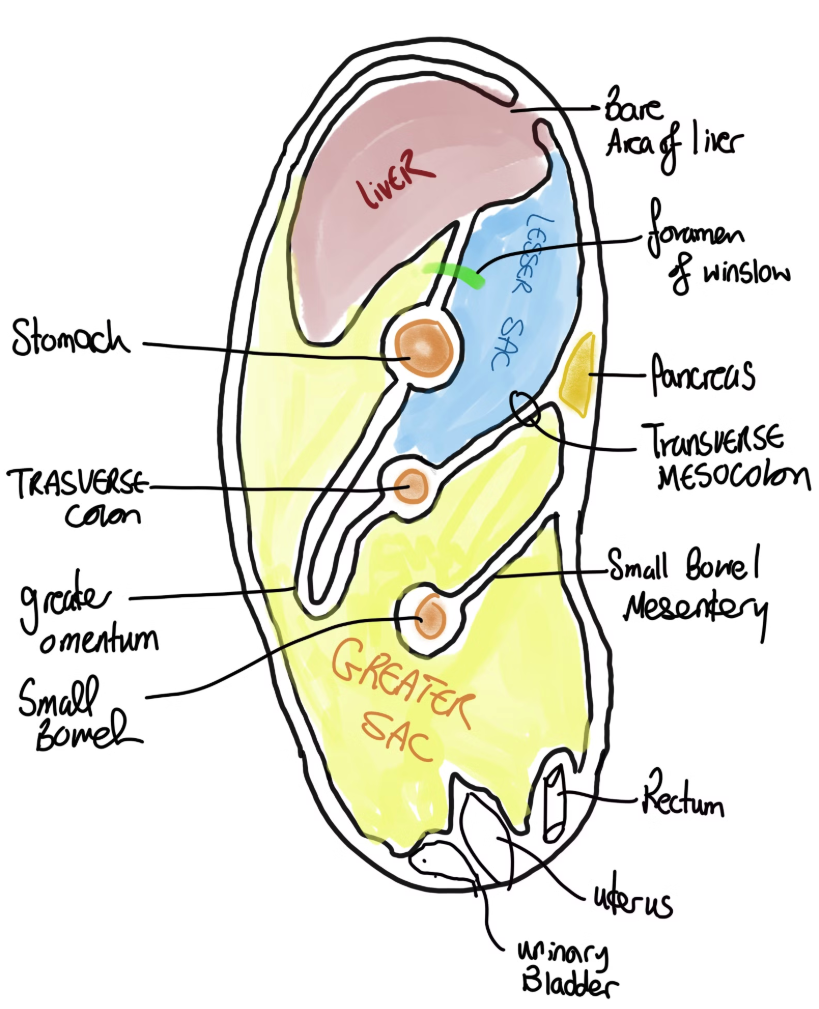
Sagittal view showing anatomical relations of the pancreas to the lesser sac and peritoneum
Relation to the SMA
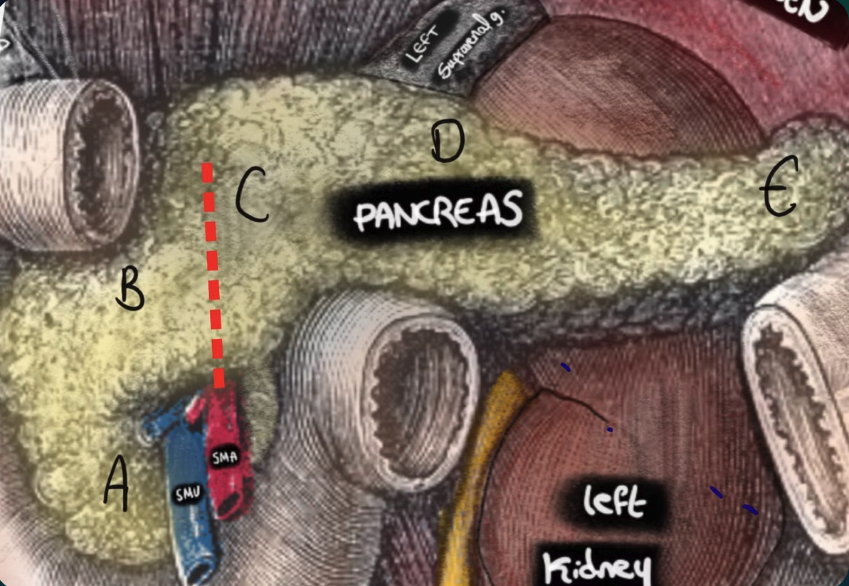
The SMA running posterior to the pancreatic neck and anterior to the uncinate process
The SMA/SMV Rule — Essential for Whipple’s and Staging
🔵 SMA and SMV run POSTERIOR to the neck — pancreas transected here in Whipple’s. The “retropancreatic tunnel” confirms resectability.
🔵 SMA and SMV run ANTERIOR to the uncinate process — the uncinate hooks behind them.
Oncological significance:
• Resectable — no contact with SMA/SMV, clear fat planes
• Borderline resectable — ≤180° contact with SMV/portal vein
• Unresectable — >180° SMA involvement, or SMV/portal vein occlusion
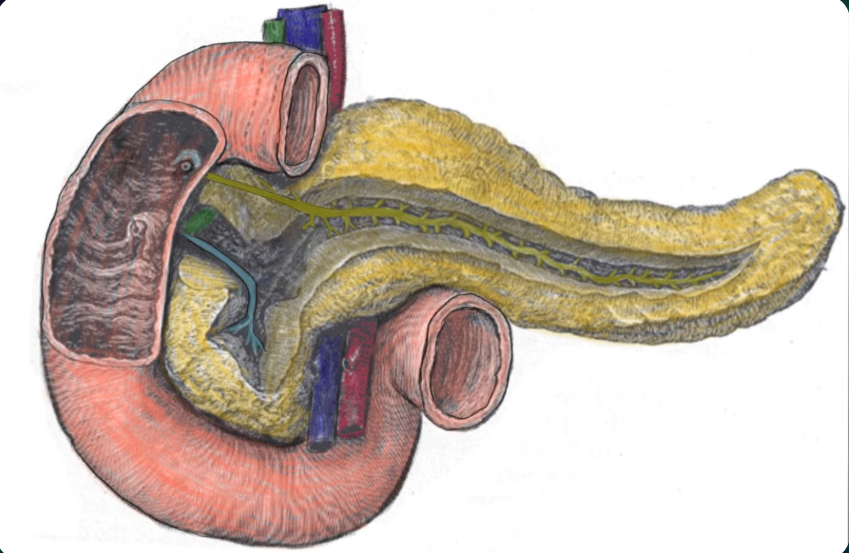
Relation to SMV, Splenic Vein and Portal Vein
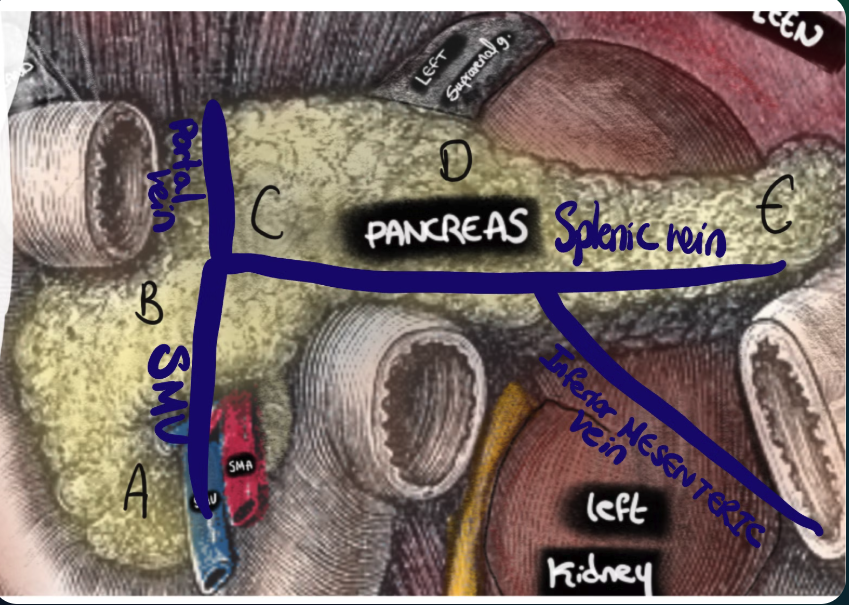
Relation of the pancreas to the portal vein, formed from the union of the SMV and splenic vein
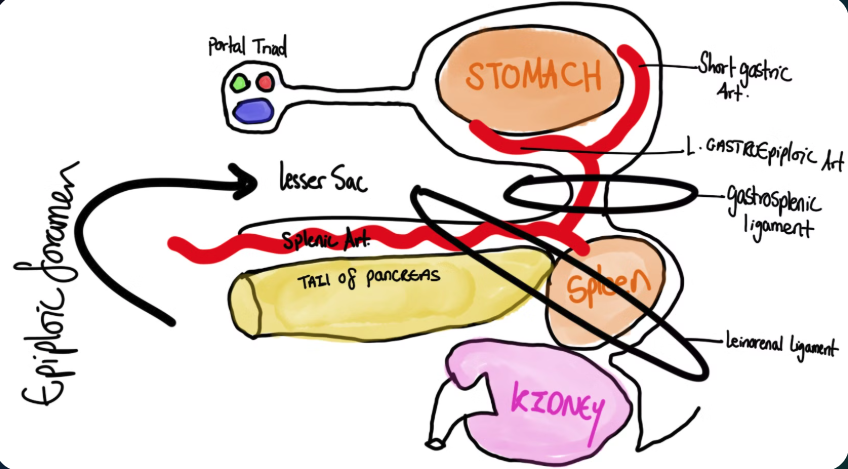
Ligamentous attachments surrounding the pancreas
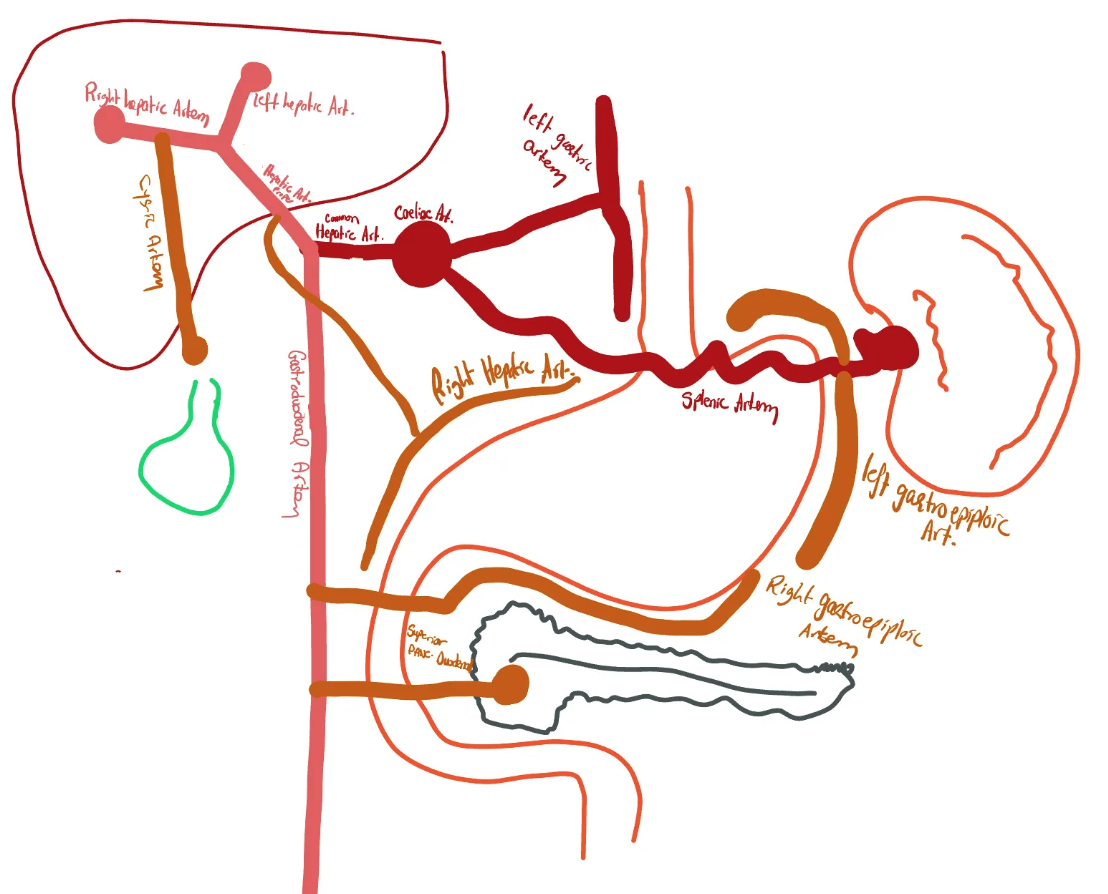
Branches of the celiac axis and pancreatic blood supply
Arterial Supply
Dual supply from coeliac axis and SMA
- Head: Superior pancreaticoduodenal artery (from GDA → coeliac axis) + Inferior pancreaticoduodenal artery (from SMA). Arcade — allows head + CBD resection without ischaemia.
- Body: Pancreatic branches of the splenic artery
- Tail: Splenic, gastroepiploic, and dorsal pancreatic arteries
Venous Drainage
All drains to portal system
- Head: Pancreaticoduodenal veins → SMV → portal vein
- Body and tail: Pancreatic veins → splenic vein
- Portal vein formation: SMV + splenic vein join behind the neck of pancreas
- Tumour involvement of SMV/portal vein = key resectability determinant
Lymphatic Drainage
Follows arterial supply
- Drains to peripancreatic lymph nodes
- Then to coeliac and superior mesenteric nodes
- Ultimately to the cisterna chyli and thoracic duct
- Involvement of coeliac axis nodes may render cancer incurable
Nerve Supply
Autonomic — pain via sympathetics
- Parasympathetic: Vagus nerve (CN X) — stimulates exocrine secretion and insulin release
- Sympathetic: Greater and lesser splanchnic nerves (T5–T10) — pain fibres travel with sympathetics, explaining epigastric pain radiating to the back
- Coeliac plexus block for refractory cancer pain
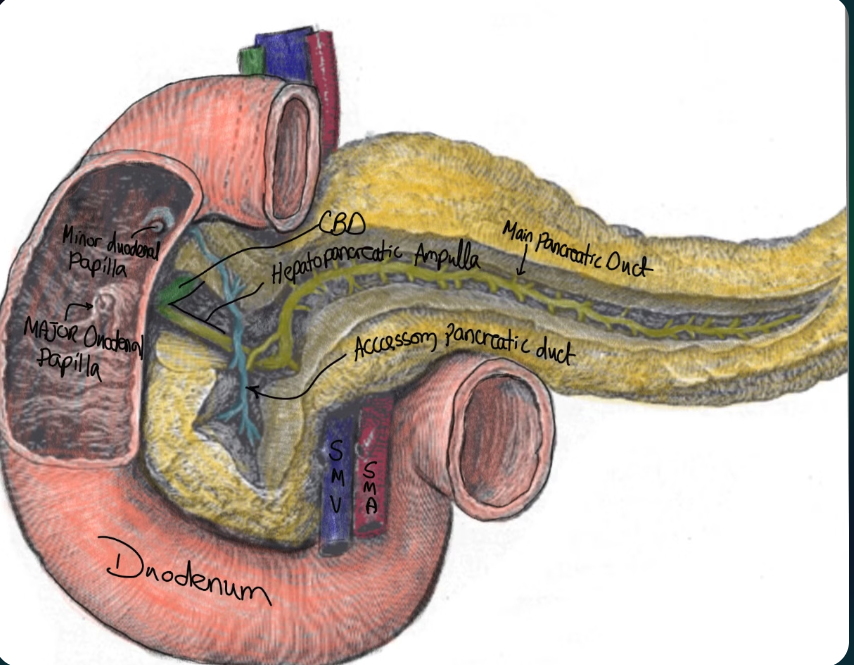
Pancreatic duct structures and drainage into the major duodenal papilla (ampulla of Vater)
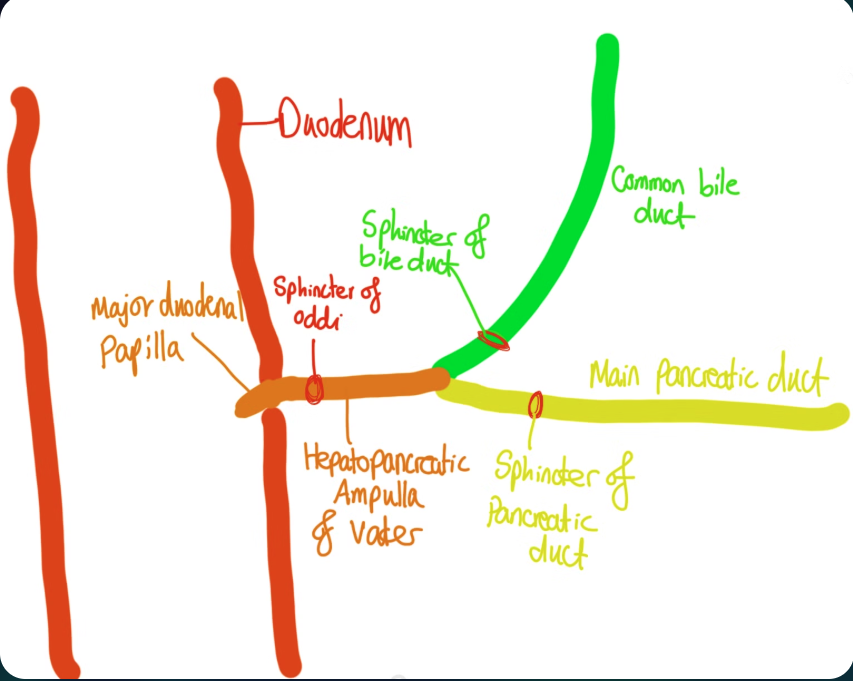
Tube-map style illustration of the biliary tree and pancreatic duct system
| Duct | Eponym | Origin | Opens at |
|---|---|---|---|
| Main pancreatic duct | Duct of Wirsung | Ventral bud | Major duodenal papilla (Ampulla of Vater) ~7cm from pylorus, via Sphincter of Oddi (joins CBD) |
| Accessory pancreatic duct | Duct of Santorini | Dorsal bud | Minor duodenal papilla (and partly into main duct). Drains lower head and uncinate process. |
Overview of pancreatic divisum
Pancreatic Divisum — Most Common Congenital Ductal Anomaly
Failure of dorsal and ventral pancreatic buds to fuse in embryological development. Most drainage must pass through the minor duodenal papilla (smaller → relative obstruction). Usually asymptomatic; associated with recurrent idiopathic pancreatitis in a subset.
Type 1 (Classic, 70%) — Complete non-fusion. Main duct → minor papilla. Accessory duct → major papilla.
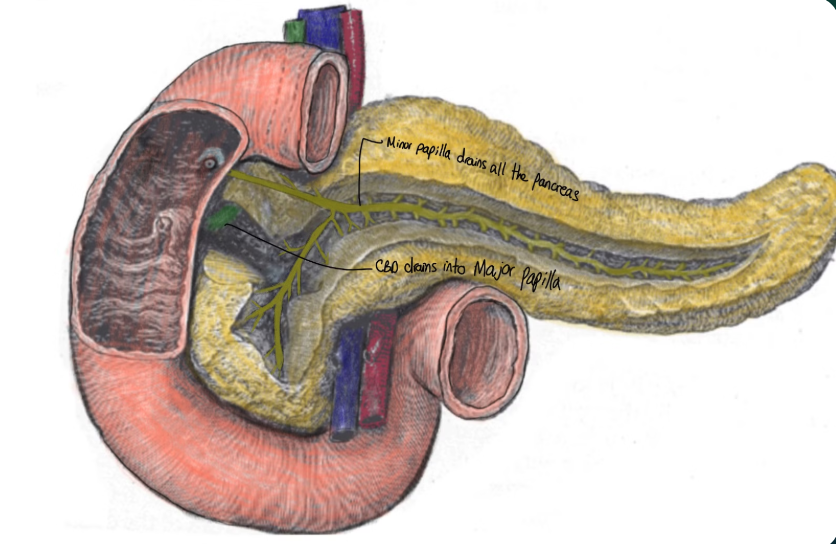
Type 2 (~20%) — Absent ventral duct. Entire pancreas drains via minor papilla.
Kocherisation is the anterior and leftward mobilisation of the second part of the duodenum by incising its lateral peritoneal attachments (the avascular fusion fascia of Treitz). Exposes the IVC and left renal vein posteriorly. The duodenum can be mobilised medially without devascularisation because the blood supply arrives medially.
Uses of Kocherisation
- Whipple’s procedure — essential first step to mobilise the pancreatic head and duodenum
- Exposing a posterior duodenal ulcer (under-running of the GDA)
- Accessing the porta hepatis and hepatoduodenal ligament
- Retroperitoneal vascular access (e.g., aortic procedures)