🟤 The Colon
Anatomy · Rectum & Anal Canal · Colorectal Cancer · Diverticular Disease · IBD · Colonic Emergencies · Lower GI Haemorrhage — MRCS Part A & B
Colonic Anatomy
The large intestine extends from the ileocaecal valve to the anal canal — approximately 1.5 metres in total length. Sections in order: caecum → ascending colon → hepatic flexure → transverse colon → splenic flexure → descending colon → sigmoid colon → rectum → anal canal.
Four external features distinguish the colon from the small bowel:
- Taeniae coli — three thickened 8 mm-wide longitudinal muscle bands running the length of the colon. They converge at the appendiceal base. Absent in the rectum (where they coalesce into a complete longitudinal muscle layer) and the appendix (which has a complete outer muscle).
- Haustra — sacculations (pouches) between the taeniae, caused by the taeniae being shorter than the bowel wall itself
- Appendices epiploicae — peritoneal fat tags hanging from the serosal surface. Can undergo torsion → epiploic appendagitis (acute LIF or RIF pain, mimics diverticulitis or appendicitis)
- Larger internal calibre — haustra cross only partially across the lumen; valvulae conniventes of the small bowel cross completely (key AXR distinction)
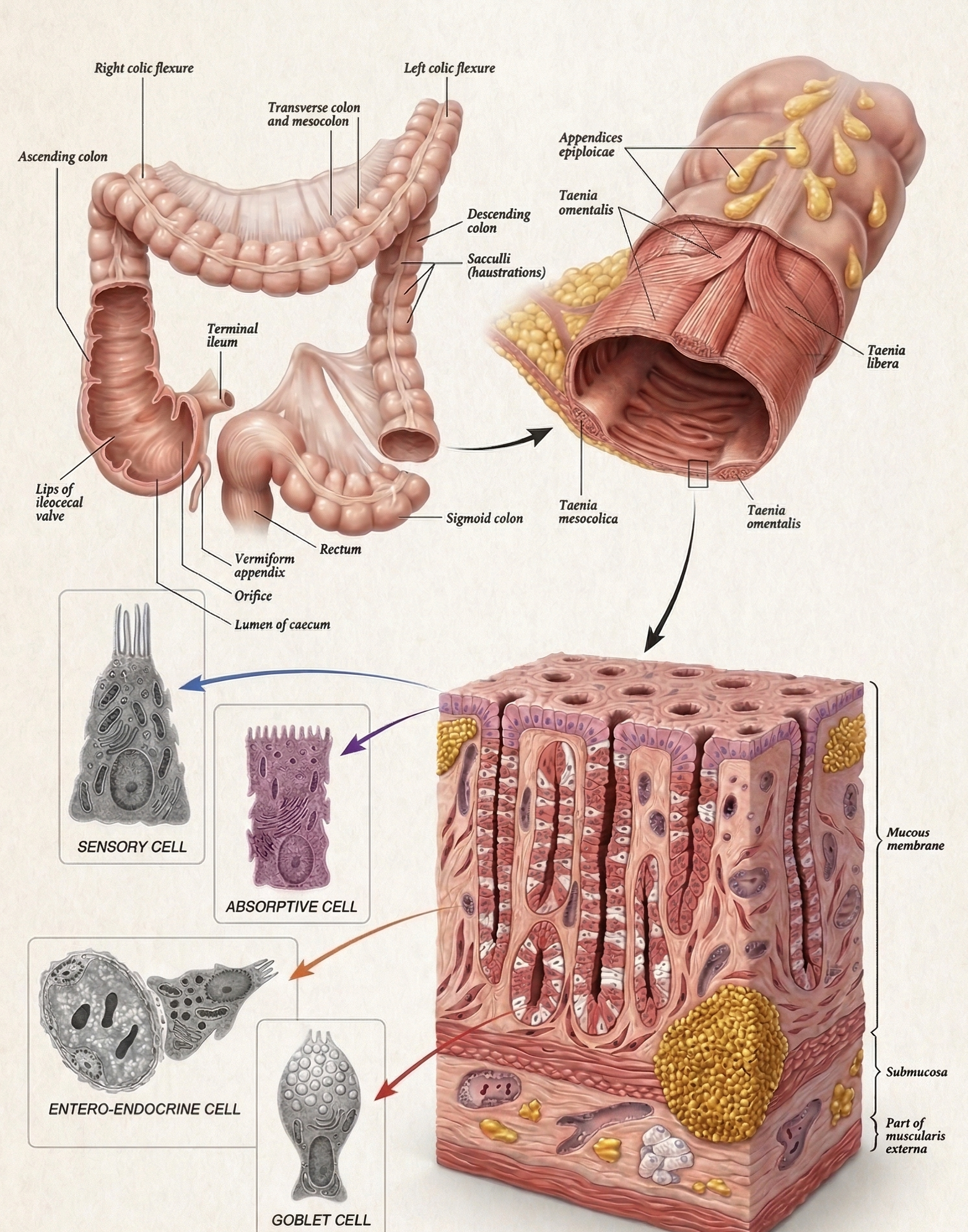
Colon — Anatomy & Histology
The characteristic external features of the colon (taeniae coli, haustra, appendices epiploicae) with the relationship between the three taeniae bands that converge at the appendiceal base. The taeniae coalesce into a complete longitudinal layer at the rectosigmoid junction. Histologically, the colon has a single-layered columnar epithelium rich in mucus-secreting goblet cells, a muscularis mucosa, submucosa, inner circular and outer (incomplete — taeniae) longitudinal muscle layers, and a serosal covering.
- Caecum
Blind pouch — right iliac fossa
First part of the large intestine. Intraperitoneal but not suspended by a mesentery. Ileocaecal valve invaginates into the caecal lumen, preventing reflux. Appendix arises from the posteromedial wall where the three taeniae coli converge.
Clinical: competent ileocaecal valve in large bowel obstruction = closed-loop obstruction → rapid pressure rise → caecal perforation (widest diameter, highest wall tension by Laplace’s law). Caecal diameter >12 cm = imminent perforation. - Ascending
Right side — hepatic flexure — retroperitoneal
Passes from the caecum to the right colic (hepatic) flexure. Primarily retroperitoneal — posterior surface lies directly on the right kidney, D2 of the duodenum, and the right ureter (critical danger structures in right hemicolectomy). Hepatic flexure relates to the inferior surface of the right lobe of the liver and the gallbladder.
- Transverse
Most mobile — transverse mesocolon — hangs between flexures
Longest and most mobile colonic segment. Suspended by the transverse mesocolon attaching to the anterior border of the pancreatic body. Greater omentum hangs from the greater curvature of the stomach and fuses anteriorly. Posterior relations: pancreatic body, D2, small bowel loops.
- Descending
Left side — retroperitoneal — left kidney and ureter
From splenic flexure to the left iliac fossa. Retroperitoneal — posterior aspect directly over the left kidney, left ureter, and left gonadal vessels. Splenic flexure is the highest point of the colon — anchored by the phrenocolic ligament to the diaphragm. Most vulnerable segment to ischaemia — watershed zone between SMA (middle colic) and IMA (left colic) territories = Griffiths’ point.
- Sigmoid
S-shaped — mobile — sigmoid mesocolon — pelvic brim at L4
Connects the descending colon to the rectum. Begins at the pelvic brim (L4 vertebral level). Highly mobile — suspended by the sigmoid mesocolon. A long sigmoid mesocolon predisposes to sigmoid volvulus. The rectosigmoid junction is identified by the termination and fusion of the taeniae coli into a complete longitudinal layer — the start of the rectum. The sigmoid mesocolon’s inverted-V root means the left ureter crosses beneath its apex — at risk in sigmoid surgery.
The blood supply reflects embryological origins. The critical transition occurs at the splenic flexure, where midgut (SMA) and hindgut (IMA) territories meet.
| Territory | Origin | Artery | Branches |
|---|---|---|---|
| Right colon (caecum → proximal 2/3 transverse colon) | Midgut | SMA | Ileocolic (caecum + appendix), right colic (ascending colon), middle colic (transverse colon) |
| Left colon (distal 1/3 transverse → sigmoid) | Hindgut | IMA | Left colic (descending colon + splenic flexure), sigmoid arteries (2–4 branches), superior rectal artery (upper rectum) |
Griffiths’ Point & Sudeck’s Point — The Two Watershed Zones
Griffiths’ point (splenic flexure): Watershed between SMA (middle colic) and IMA (left colic) territories. The most vulnerable area to ischaemia — particularly when the IMA is ligated (during AAA repair, left colonic surgery, or sigmoid resection). Ischaemic colitis at the splenic flexure is the most common presentation.
Sudeck’s point: Junction between the sigmoid arteries and the superior rectal artery. If the IMA is ligated below Sudeck’s point during anterior resection, the sigmoid colon loses its blood supply → ischaemia of the sigmoid. The IMA must be ligated above the sigmoid arteries (high tie) for oncological reasons, but the anastomosis must receive adequate blood supply from the marginal artery.
Marginal artery of Drummond: A continuous arterial arcade running along the mesenteric border of the entire colon, connecting the SMA and IMA territories. Provides the critical collateral supply at the watershed zones. However, the arcade is often poorly developed at Griffiths’ point — explaining the vulnerability of the splenic flexure.
| Segment | Venous Drainage | Ultimately to |
|---|---|---|
| Right colon | Superior mesenteric vein (SMV) | Portal vein → liver |
| Left colon + sigmoid | Inferior mesenteric vein (IMV) → splenic vein | Portal vein → liver |
| Upper rectum | Superior rectal vein → IMV → portal vein | Portal system |
| Middle/lower rectum & anal canal | Middle + inferior rectal veins → internal iliac → IVC | Systemic (IVC) |
The rectum is therefore a portosystemic anastomosis — in portal hypertension, blood is diverted via the superior rectal → middle/inferior rectal pathway → rectal varices (distinct from haemorrhoids). This also means rectal cancer may spread via two venous routes — to the liver (portal) and to the lungs (systemic via IVC).
Lymphatics
Lymphatic drainage follows the arterial supply: epicolic nodes (on the colon wall) → paracolic nodes (along the marginal artery) → intermediate mesenteric nodes (along named arteries) → principal/pre-aortic nodes (at the SMA and IMA origins) → cisterna chyli (at L1/L2) → thoracic duct. Relevant for surgical oncology — lymph node clearance must include the named arterial pedicle at its origin.
Nerve Supply
- Parasympathetic: Vagus nerve (CN X) supplies the colon to the splenic flexure (the midgut/hindgut boundary). Pelvic splanchnic nerves (S2, S3, S4 — the nervi erigentes) supply the left colon and rectum. Stimulates peristalsis and secretion.
- Sympathetic: Superior mesenteric plexus (right colon), inferior mesenteric plexus (left colon + sigmoid), hypogastric plexus (rectum). Inhibit peristalsis. The hypogastric plexus lies on the pelvic side wall and in front of the sacrum — at risk in TME, anterior resection, and APR → bladder dysfunction (neurogenic bladder) and sexual dysfunction (erectile dysfunction, retrograde ejaculation, dry orgasm).
- Enteric nervous system: Myenteric plexus (Auerbach’s — motility) and submucosal plexus (Meissner’s — secretion). Functions independently of the ANS.