🔵 Anal Canal — Anatomy & Pathology
Anatomy of the anal canal and sphincter complex; haemorrhoids; anal fistula and Parks’ classification; pilonidal sinus; anal fissure; and anal canal tumours.
Anal Canal Anatomy
The anal canal is approximately 4 cm long, extending from the anorectal junction (proximally) to the anal verge (distally). It is divided into two functional and embryological zones by the dentate line (pectinate line). Below the dentate line, a further subdivision is made by Hilton’s white line (squamous mucocutaneous junction).
| Feature | Above dentate line (upper 2/3) | Below dentate line (lower 1/3) |
|---|---|---|
| Epithelium | Columnar epithelium (transitional / cloacogenic zone near the dentate line itself) |
|
| Embryological origin | Hindgut endoderm | Ectoderm (proctodeum) |
| Sensory innervation | Autonomic (inferior hypogastric plexus) — pain poorly localised; visceral. Injections above the dentate line are essentially painless. | Somatic (pudendal nerve — inferior rectal branch) — exquisitely sensitive. Injections below the dentate line cause severe pain. |
| Arterial supply | Superior rectal artery (branch of IMA — inferior mesenteric artery) | Middle and inferior rectal arteries (branches of internal pudendal artery from the internal iliac artery) |
| Venous drainage | Superior rectal vein → IMV → splenic vein → portal venous system | Middle and inferior rectal veins → internal iliac veins → IVC. This junction is a portosystemic anastomosis — clinically relevant in portal hypertension (anorectal varices). |
| Lymphatic drainage | Internal iliac lymph nodes (perirectal and paravertebral nodes) | Superficial inguinal lymph nodes and femoral nodes — explains why anal SCC metastasises to the groin |
| Tumour type | Adenocarcinoma (if above dentate line, behaves like rectal cancer) | Squamous cell carcinoma (most common), and squamous-type precursor lesions (AIN) |
Below the dentate line, a further subdivision is made by Hilton’s white line (the squamous mucocutaneous junction), visible as a pale line approximately halfway between the dentate line and the anal verge:
- Zona haemorrhagica (between dentate line and Hilton’s white line): stratified squamous non-keratinised epithelium (“anoderm”). This zone overlies the internal haemorrhoidal plexus.
- Zona cutanea (below Hilton’s white line to the anal verge): stratified squamous keratinised epithelium, blending gradually with the perianal skin.
Tumour Classification by Zone — Canal vs Margin
The squamous mucocutaneous junction (Hilton’s white line) determines how anal tumours are classified:
🔵 Tumours above Hilton’s white line (arising from mucosa — glandular, transitional, or non-keratinising squamous epithelium) → called anal canal cancer
🔵 Tumours below Hilton’s white line (arising from skin or distal to the squamous mucocutaneous junction) → called anal margin cancer
This distinction matters because anal margin cancers are managed differently — T1 anal margin SCCs can be treated with wide local excision, whereas anal canal SCCs (regardless of T stage) are treated with definitive chemoradiotherapy.
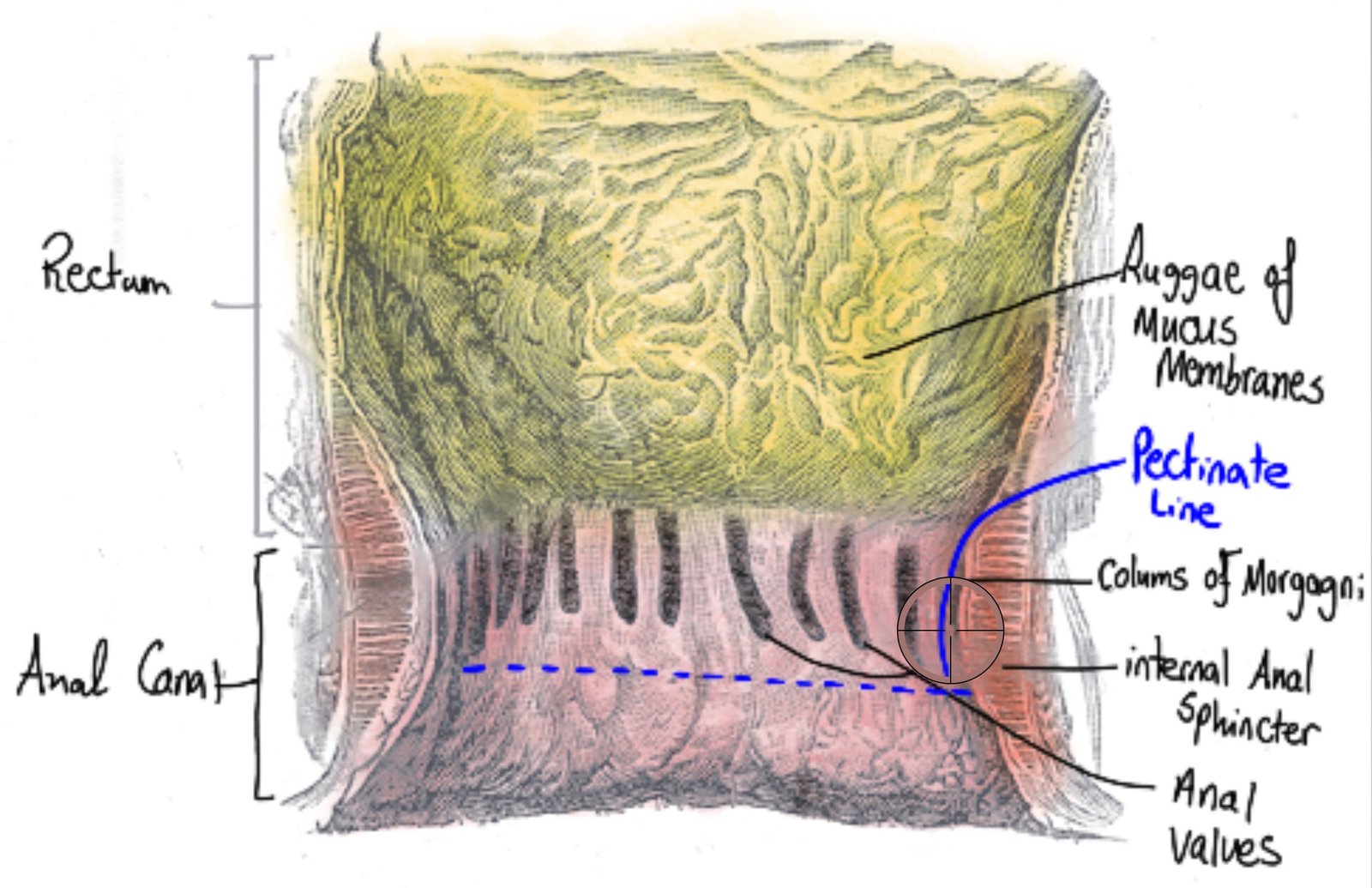
Anatomical diagram showing the anal canal and the dentate line.
-
Internal sphincter
Internal Anal Sphincter (IAS) — involuntary, circular, smooth muscle
A thickening of the inner circular smooth muscle layer of the rectum as it enters the anal canal. Extends from the anorectal junction to approximately 1 cm below the dentate line. Composed of non-striated (smooth) involuntary muscle supplied by autonomic nerves (sympathetic — contracts; parasympathetic — relaxes).
- Responsible for approximately 85% of resting anal tone — the major barrier against passive faecal incontinence
- The rectoanal inhibitory reflex (RAIR): rectal distension → reflex IAS relaxation → allows the sensory-rich upper anal canal (transition zone) to “sample” rectal contents → conscious decision to defer or allow defaecation
- RAIR is absent in Hirschsprung’s disease (no ganglionic cells)
- IAS disruption (e.g. after internal sphincterotomy, instrumentation, forceps delivery) → passive faecal incontinence
-
External sphincter
External Anal Sphincter (EAS) — voluntary, striated, skeletal muscle
A cylinder of striated (skeletal) voluntary muscle surrounding the IAS, supplied by the pudendal nerve (S2–S4 — inferior rectal branch). Extends from the perineal body anteriorly and the anococcygeal ligament posteriorly, running the full length of the anal canal.
- Responsible for voluntary squeeze pressure — the extra contractile force when continence is threatened (“the squeeze”)
- EAS damage (obstetric trauma — third/fourth degree tears, APR, sphincterotomy) → urge faecal incontinence and inability to defer defaecation
- Assessed on clinical examination as “squeeze tone” (ask patient to squeeze) — contrasted with resting tone (IAS-dependent)
-
Puborectalis
Puborectalis Muscle — the anorectal angle
Part of the levator ani complex. A U-shaped loop of striated muscle passing from the pubic bone around the posterior anorectal junction, pulling the junction anteriorly and creating the anorectal angle (approximately 90°). The superior part of the external sphincter fuses with puborectalis.
- The anorectal angle is essential for continence — it creates a flap-valve mechanism whereby raised intraabdominal pressure (coughing, straining) increases the occlusion of the anterior rectal wall against the posterior wall rather than opening the canal
- During normal defaecation, the puborectalis relaxes → anorectal angle increases → the canal straightens → faecal passage is facilitated
- Paradoxical contraction of puborectalis during attempted defaecation = anismus (obstructed defaecation syndrome) — treated with biofeedback
- Supplied by direct branches of S3–S4 (not the pudendal nerve) — this distinction is clinically important in nerve-sparing pelvic surgery
-
Longitudinal muscle
Longitudinal Muscle Layer — the supporting scaffold
Extensions from the outer longitudinal muscle layer of the rectum pass downward between the IAS and EAS, giving off fibrous septa that interdigitate with both sphincters and extend into the perianal skin (corrugator cutis ani) and perianal fat. These extensions:
- Support and bind the sphincter complex as an integrated functional unit
- Form the intersphincteric space — the plane between IAS and EAS. Cryptoglandular infections originate here (→ anal abscesses → fistulas)
- The fibrous septa anchor skin to the underlying sphincter — producing the characteristic “corrugated” appearance of the anoderm
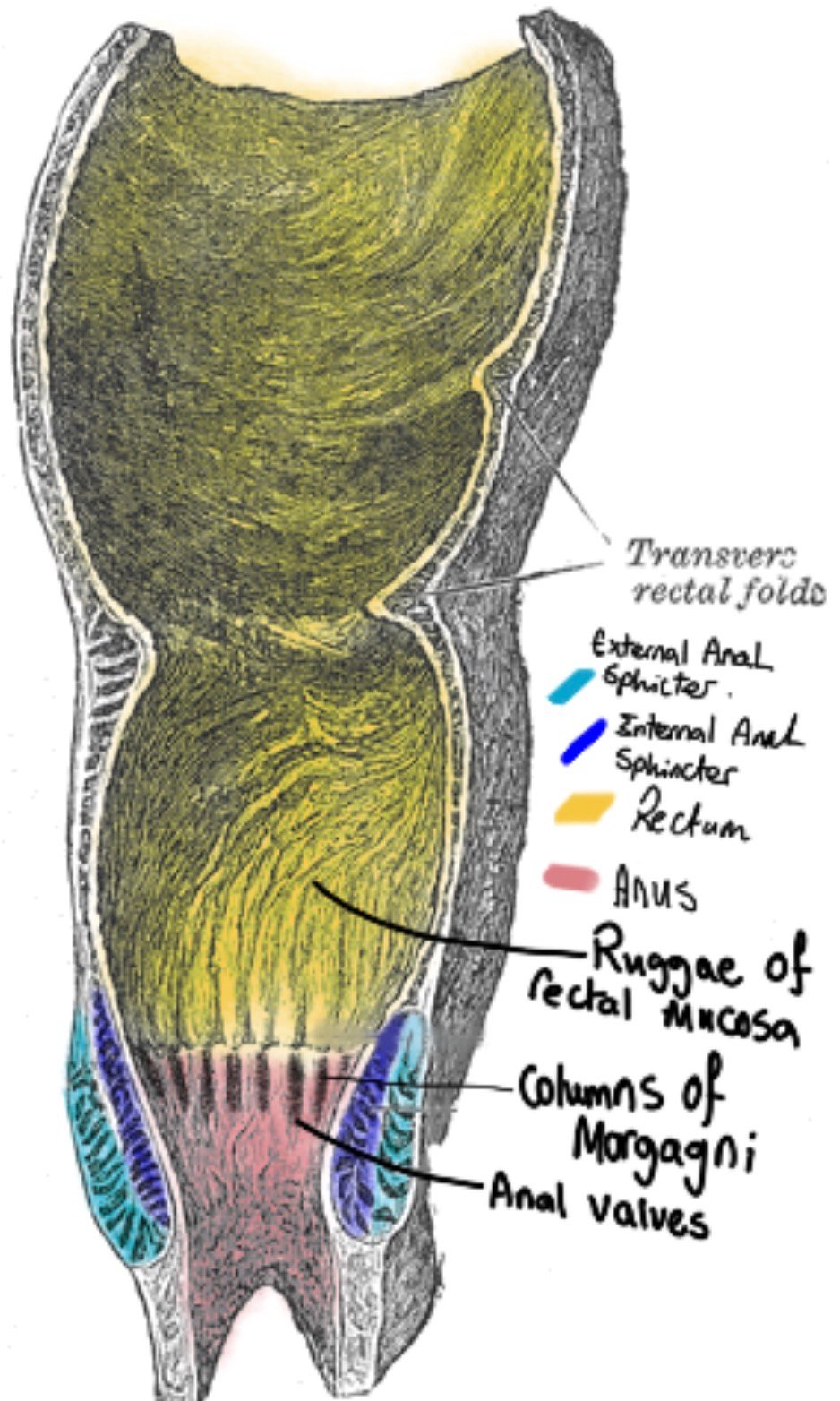
Diagram showing the anal sphincter complex and rectal folds.
The Four Mechanisms of Faecal Continence
Continence is not a single mechanism — it requires all four components working in concert:
🔵 Internal anal sphincter (IAS): Maintains resting tone (85% of resting pressure). Prevents passive leakage between defaecations.
🔵 External anal sphincter (EAS) + puborectalis: Voluntary squeeze to defer defaecation when urgency arises. Only sustainable for ~60 seconds before fatigue.
🔵 Anorectal angle: The puborectalis flap-valve — raised intraabdominal pressure increases occlusion rather than expulsion.
🔵 Rectal reservoir: The capacitance of the rectum allows stool storage. Loss of the rectal reservoir (after LAR + TME) causes LARS — frequency, urgency, clustering, soiling despite intact sphincters.
The St Mark’s continence assessment: Wexner score (0–20) or Cleveland Clinic Incontinence Score quantifies severity of faecal incontinence across five domains. Guides management (biofeedback → sacral nerve stimulation → sphincter repair → colostomy as last resort).