🟠 Anterior Abdominal Wall
Layers · Muscles · Fasciae · Rectus Sheath · Peritoneum · Nerves · TAP Block · Vessels · Abdominal Planes — MRCS Part A & B
Layers of the Anterior Abdominal Wall
The anterior abdominal wall consists of nine layers from superficial to deep. Knowing these in order is fundamental for surgical access, hernia repair, and regional anaesthesia.
- 1
Skin
Langer’s lines run transversely in the lower abdomen — basis for the cosmetic advantage of Pfannenstiel, Lanz, and other transverse incisions over vertical ones.
- 2
Subcutaneous Fat
Variable thickness. Thickened in obesity — increases difficulty of laparoscopic port insertion and open wound closure.
- 3
Camper’s Fascia — Superficial Fatty Layer
The superficial fatty layer of the superficial fascia. Continues onto the penis and scrotum. No significant deep attachments — freely mobile fat layer.
- 4
Scarpa’s Fascia — Deep Membranous Layer
The deep membranous layer of the superficial fascia. Key: attaches to the deep fascia of the thigh 2.5 cm below the inguinal ligament, preventing spread of fluid (urine, infection) into the thigh. Continues into the perineum as Colles’ fascia, and onto the penis/scrotum as dartos fascia.
- 5
External Oblique Muscle / Aponeurosis
Most superficial flat muscle. Fibres run inferomedially (“hands in front pockets”). Inferior margin forms the inguinal ligament (ASIS → pubic tubercle).
- 6
Internal Oblique Muscle / Aponeurosis
Deep to external oblique. Fan-shaped fibres — superior fibres perpendicular, inferior fibres parallel to external oblique. Aponeurosis splits around the rectus above the arcuate line.
- 7
Transversus Abdominis Muscle / Aponeurosis
Deepest flat muscle. Fibres run horizontally (like a corset). Forms the TAP plane with the internal oblique — where thoracoabdominal nerves travel and TAP block is deposited.
- 8
Transversalis Fascia
Thin continuous layer lining the deep surface of transversus abdominis. Forms the deep inguinal ring (a defect in this layer) and contributes the internal spermatic fascia of the cord.
- 9
Parietal Peritoneum
Somatic innervation (T7–L1) — acutely sensitive to localised pain, temperature, pressure. Visceral peritoneum = autonomic innervation → vague, poorly localised pain. This distinction explains the migration of pain in appendicitis.
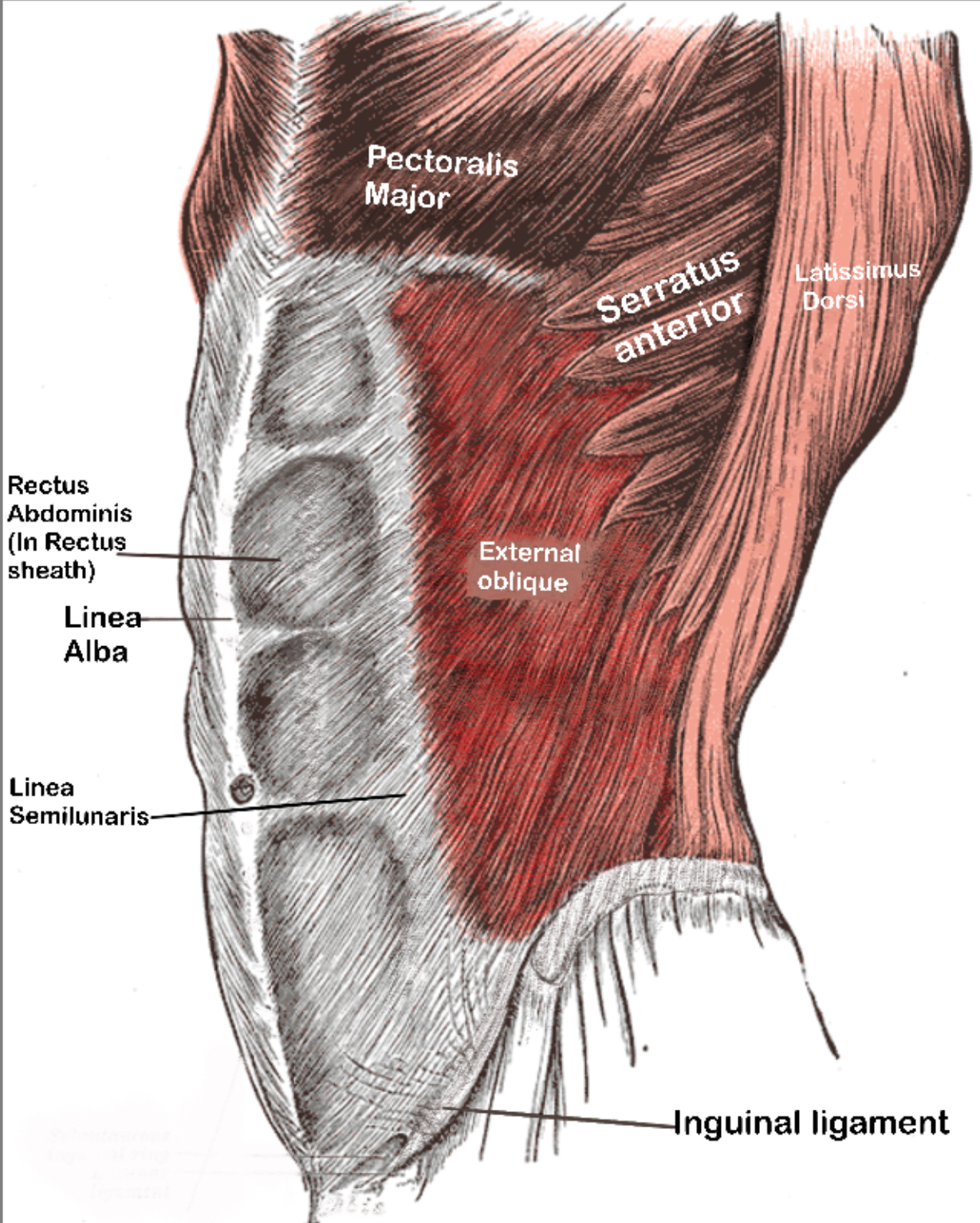
External Oblique Muscle
Origin: external surfaces of ribs 5–12. Fibres run inferomedially — “hands in front pockets” direction. The inferior margin thickens and rolls inward to form the inguinal ligament from the ASIS to the pubic tubercle. The aponeurosis forms the anterior wall of the rectus sheath and the superficial inguinal ring.
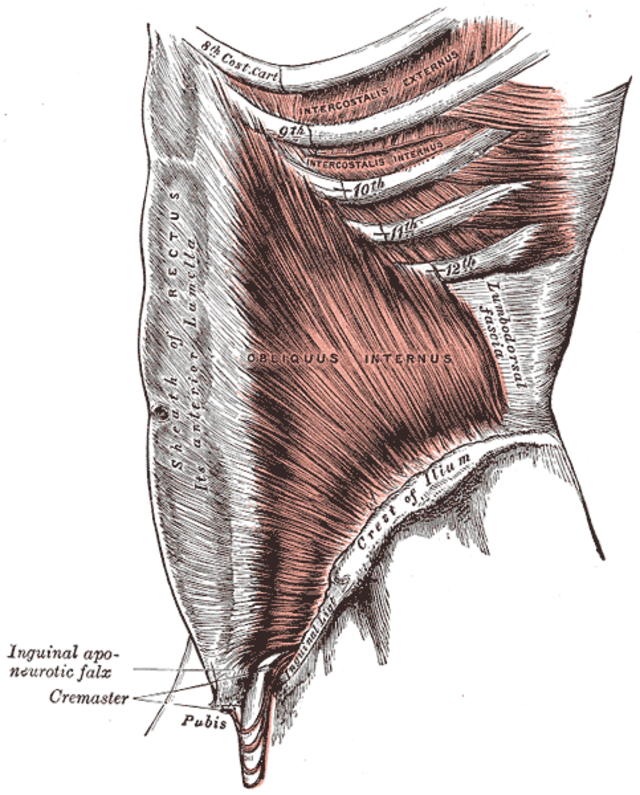
Internal Oblique Muscle
Origin: thoracolumbar fascia, anterior 2/3 of iliac crest. Fibres are fan-shaped — superior fibres run perpendicular to the external oblique; inferior fibres are parallel. The aponeurosis splits above the arcuate line to form both the anterior and posterior rectus sheath. Below the arcuate line, all fibres pass anterior. Contributes to the conjoint tendon with transversus abdominis — reinforcing the posterior wall of the inguinal canal medially.
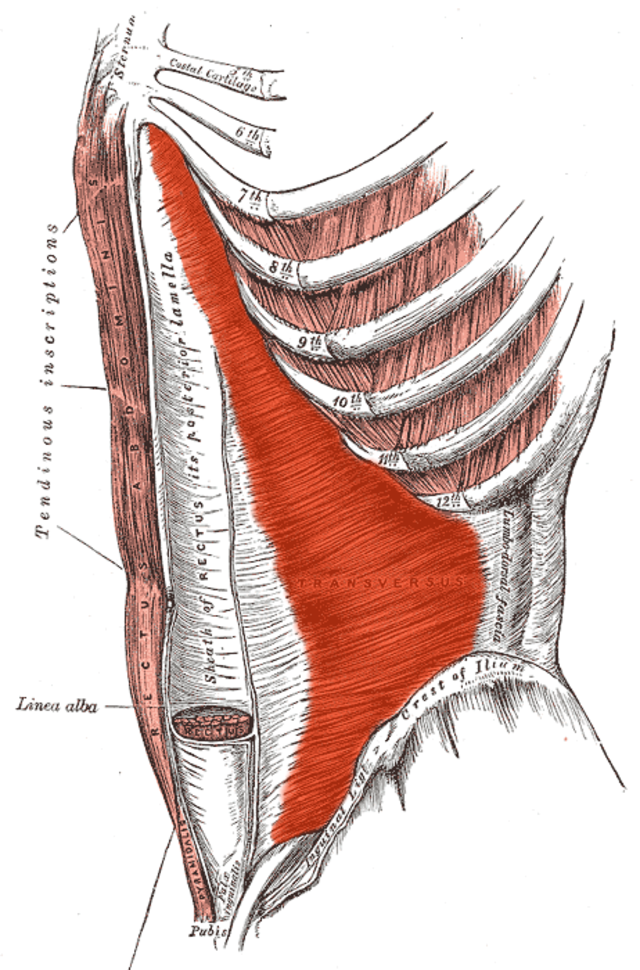
Transversus Abdominis Muscle
Origin: internal surfaces of ribs 7–12, thoracolumbar fascia, iliac crest. Fibres run horizontally — the “corset” muscle, most important for intraabdominal pressure maintenance. Forms the TAP plane with the internal oblique above it. Below the arcuate line its aponeurosis also passes entirely anterior. Contributes to the conjoint tendon.