🟣 The Spleen
Anatomy and physiology; splenic disease; trauma grading and management; splenectomy; OPSI — MRCS Part A & B high-yield notes.
Splenic Anatomy
The spleen is the largest lymphoid organ in the body — entirely intraperitoneal, derived from mesenchymal tissue in the dorsal mesogastrium. It measures approximately 12 × 7 × 4 cm and weighs 150–200 g in a healthy adult.
- Located in the left hypochondrium, protected by ribs 9–11 posteriorly
- Long axis lies parallel to the 10th rib, running obliquely from T10 to the anterior axillary line
- Normally not palpable — must approximately double in size before crossing the left costal margin
- Has a palpable notch on its lower medial border — felt when the spleen is enlarged
- Has four surfaces: gastric (anteromedial), renal (posteromedial), colic (inferior), diaphragmatic (superolateral)
Direction of Splenomegaly — Why Start in the RIF?
The phrenicocolic ligament tethers the inferior pole of the spleen, preventing straightforward caudal expansion. As the spleen enlarges, it is directed obliquely downward and medially towards the right iliac fossa. This is why palpation for splenomegaly must begin in the right iliac fossa and sweep diagonally upward to the left costal margin — starting at the left costal margin risks missing the leading edge.
A spleen is distinguished from an enlarged left kidney by: inability to get above it, it is not ballottable, moves with inspiration, has a palpable notch, and is dull to percussion (a kidney is resonant anteriorly).
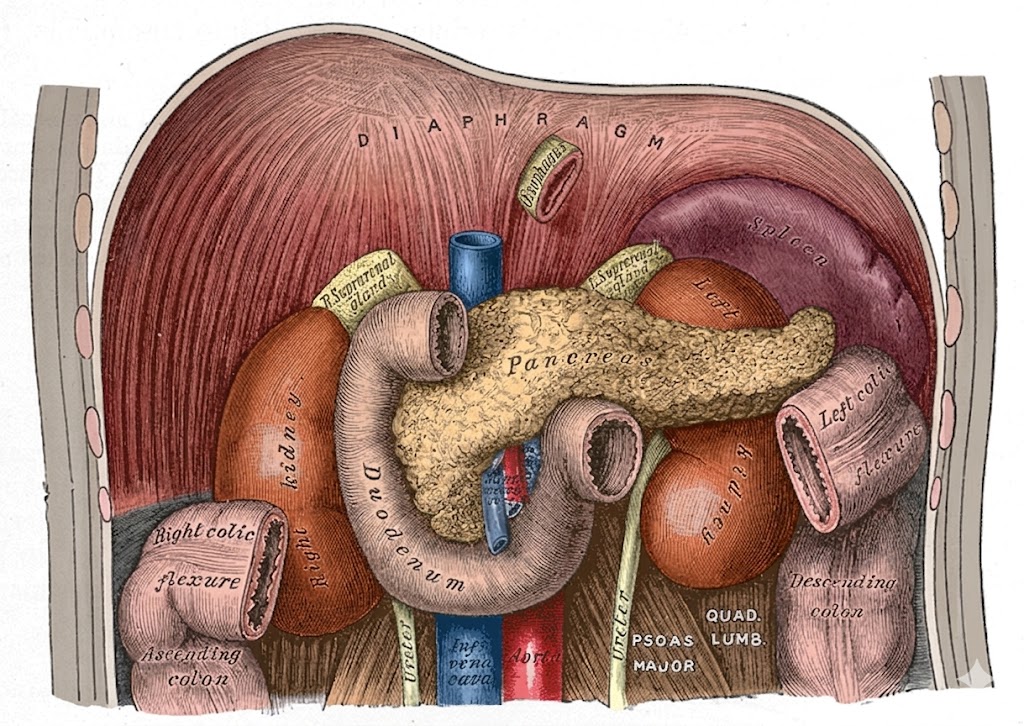
Relations of the Spleen to Adjacent Organs
The spleen sits in the left hypochondrium in close relation to the stomach (anteromedially — gastrosplenic ligament), left kidney (posteromedially — splenorenal ligament), splenic flexure of colon (inferiorly — phrenicocolic ligament), tail of pancreas (at the hilum within the splenorenal ligament), and the diaphragm superolaterally.
The spleen is suspended by four peritoneal folds. Their contents are a favourite exam topic, particularly the splenorenal and gastrosplenic ligaments.
🔗 Gastrosplenic Ligament
Connects the spleen to the greater curvature of the stomach. The anterior fold of the dorsal mesogastrium.
⚠️ Division during splenectomy must avoid the greater curvature — too close = gastric devascularisation
🔗 Splenorenal (Lienorenal) Ligament
Connects spleen to the left kidney/posterior abdominal wall. The posterior fold of the dorsal mesogastrium.
🚨 Blind hilar clamping → pancreatic tail injury → postoperative pancreatic fistula
🔗 Phrenicosplenic (Phrenicocolosplenic) Ligament
Connects spleen to the diaphragm superiorly.
Divided during splenectomy to fully mobilise the upper pole. Risk of diaphragmatic tear with massive adherent spleens.
🔗 Splenocolic (Phrenicocolocolic) Ligament
Connects spleen to the splenic flexure of the colon inferiorly.
Divided during mobilisation of the inferior pole. Risk of left colonic injury if traction is excessive.
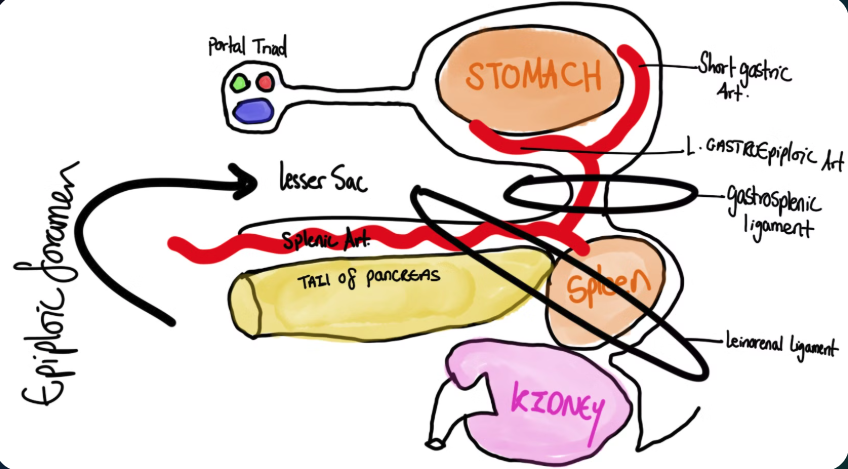
Splenorenal Ligament — Pancreatic Tail at the Hilum
The tail of the pancreas lies within the splenorenal ligament and may extend directly to the splenic hilum. This diagram illustrates the close anatomical relationship between the splenic vessels and the pancreatic tail — the key reason why blind clamping at the hilum during splenectomy risks pancreatic tail injury and postoperative pancreatic fistula.
Splenic Arterial & Venous Supply
The splenic artery arises as the largest branch of the coeliac trunk and follows a tortuous course along the superior border of the pancreas before entering the splenorenal ligament. The splenic vein runs posterior to the pancreatic body and tail, joining the superior mesenteric vein behind the neck of the pancreas to form the portal vein. The pancreaticoduodenal arcade provides the dual supply to the pancreatic head.
Kehr’s Sign — Referred Left Shoulder Tip Pain
The superior surface of the spleen is related to the left diaphragm. The diaphragm is innervated by the phrenic nerve (C3, C4, C5). Intraperitoneal blood (from splenic rupture or haemorrhage) or inflamed splenic tissue irritating the left hemidiaphragm causes the brain to misinterpret the afferent signal as originating from the left shoulder tip (supraclavicular nerves, C3–C5) — this is Kehr’s sign.
Classically elicited in the Trendelenburg position (head down), which allows blood to pool under the left diaphragm. A positive Kehr’s sign in the context of abdominal trauma = splenic injury until proven otherwise.
Found in 10–30% of the population. Most common locations in order of frequency:
- Splenic hilum (most common, ~75%)
- Gastrosplenic ligament
- Greater omentum
- Splenorenal ligament, along splenic vessels, in the tail of pancreas
Accessory Spleens in ITP — Must Find All of Them
In immune thrombocytopenic purpura (ITP), splenectomy is performed to remove the site of platelet destruction. If accessory spleens are missed, residual splenic tissue resumes platelet destruction → disease relapse. The hilum, gastrosplenic ligament, and omentum must be systematically searched and all accessory spleens removed. This is one of the most common causes of “failed” splenectomy for ITP.