🫘 Ureteric Anatomy & Relations
Course, constrictions, crossings, and the high-yield surgical relations that appear repeatedly in the MRCS.
🗺️ The Course of the Ureter
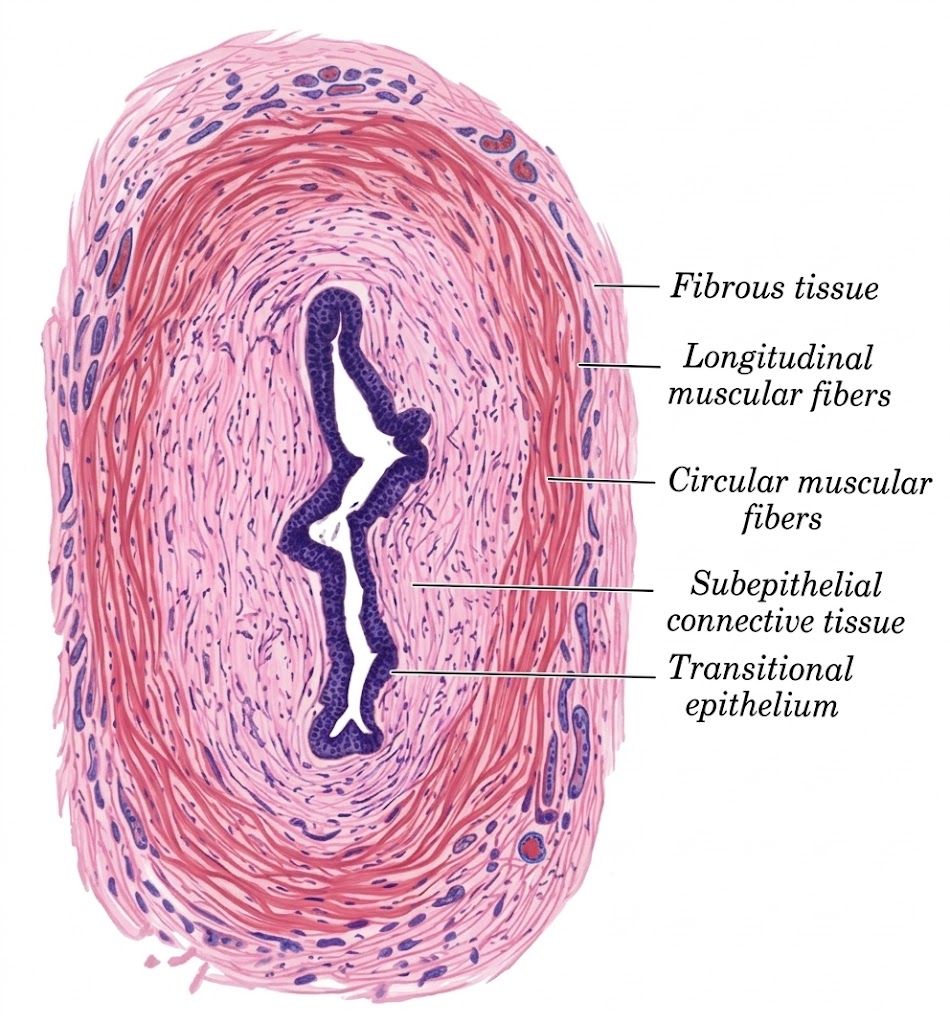
The ureter is a muscular tube approximately 25–30 cm long, running from the renal pelvis to the posterolateral angle of the bladder. It is entirely retroperitoneal throughout its course. Its wall has an inner transitional epithelium, a middle muscularis (inner longitudinal + outer circular smooth muscle), and an outer adventitia.
It can be divided into an abdominal part (renal pelvis to pelvic brim) and a pelvic part (pelvic brim to bladder). Urine is propelled by peristalsis — rhythmic coordinated contraction of the smooth muscle, not gravity. This is why obstruction causes colicky pain and why urine can still drain against gravity.
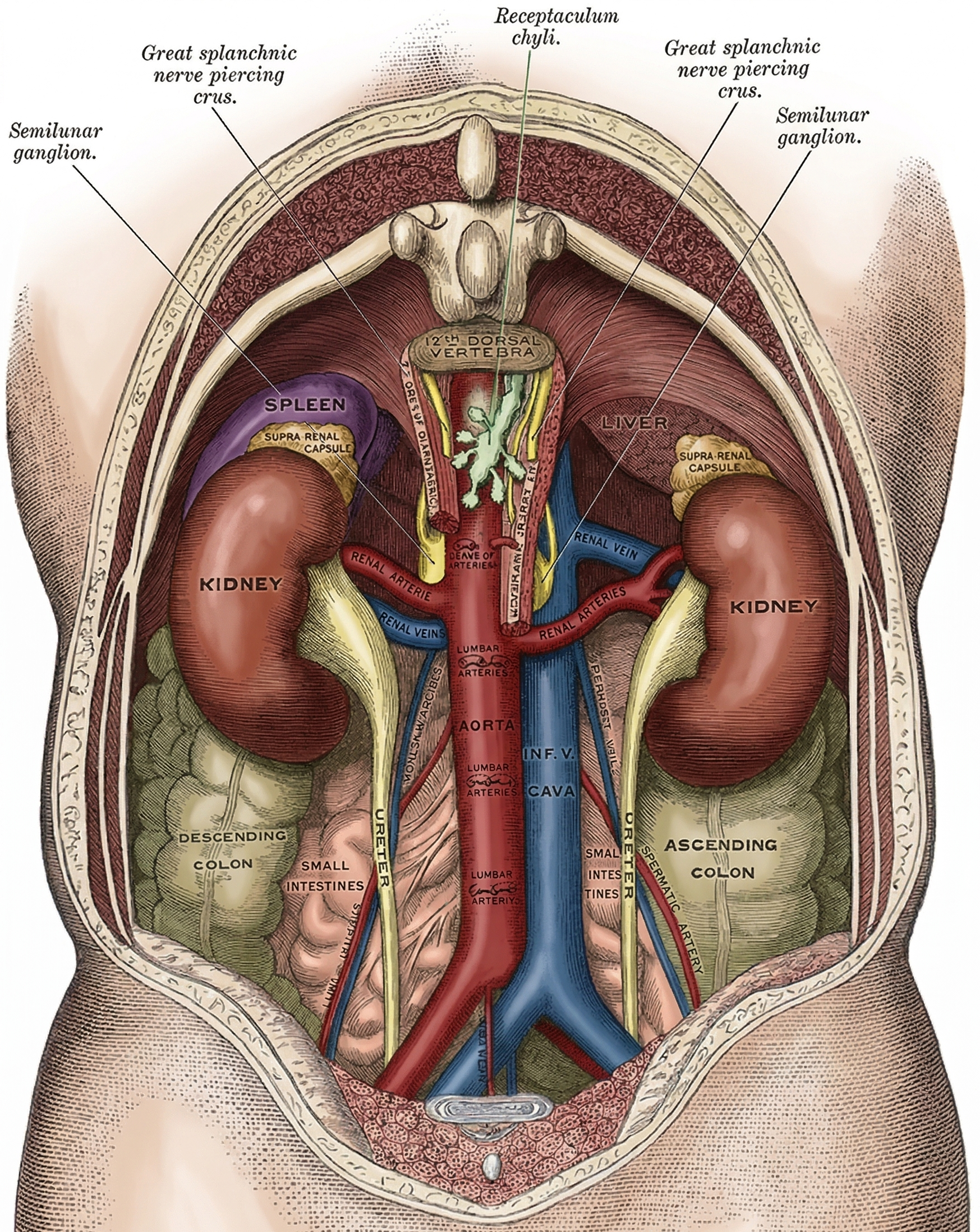
In its abdominal course, the ureter lies on the medial part of psoas major, behind the peritoneum. It is crossed obliquely by the gonadal vessels (testicular or ovarian). The right and left ureters differ in their immediate anterior relations:
Once it crosses the pelvic brim, the ureter runs downward along the lateral pelvic wall, anterior to the hypogastric (internal iliac) artery and medial to the obturator nerve. It then turns anteromedially toward the bladder.
In the male, the vas deferens loops over the external iliac vessels and then crosses medial to the ureter near the bladder — the ureter and vas deferens cross just before entering the bladder. The seminal vesicle lies just anterior to the ureter’s entry point.
In the female, the ureter forms the posterior boundary of the ovarian fossa on the lateral pelvic wall. It then runs medially on the lateral aspect of the cervix and upper vagina. The uterine artery accompanies it for ~2.5 cm before crossing anteriorly — the classic “water under the bridge” relation (~2 cm lateral to the cervix).
The Ureter Is Identified by Its Peristalsis
Intraoperatively, the ureter can be confused with the gonadal vessels. The key distinguishing feature is peristalsis — gentle pinching of the ureter causes a visible peristaltic wave to propagate along it. The gonadal vessels do not peristalse. The ureter also has a characteristic white glistening appearance with a faint longitudinal vascularity. This is a classic MRCS viva point.
Blood Supply — The “Multiple Sources” Principle
The ureter has a segmental blood supply from multiple sources. It is critical to understand that the vessels approach from the medial side in the abdomen and the lateral side in the pelvis — so surgical dissection should always be on the opposite side to avoid devascularisation.
Ureteric Devascularisation
Stripping the periureteric adventitia during dissection removes the longitudinal vascular plexus running within it. This is a common cause of delayed ureteric necrosis and stricture after pelvic surgery. Always preserve the periureteric tissue. Mobilise only what is necessary, and stay away from the medial side in abdominal dissection and the lateral side in pelvic dissection.
Nerve Supply — Why It Causes Colic
The ureter is innervated by T10–L1 (autonomic fibres via the renal, aortic, and hypogastric plexuses). Sensory pain fibres travel with sympathetic fibres back to T10–L2 spinal levels. This explains why ureteric colic classically radiates from loin to groin — and why pain may radiate to the inner thigh (genitofemoral nerve, L1–L2) or scrotum / labium majus (ilioinguinal nerve).
The ureteric wall has three coats. Understanding the muscular arrangement is useful for explaining peristalsis and why the ureter can be identified intraoperatively by pinching it.
(Fibrous coat)
(Muscular coat)
(Mucous coat)
Transitional Cell Carcinoma — Why the Urothelium Matters
The entire urinary tract from renal pelvis → ureter → bladder → proximal urethra is lined by transitional epithelium (urothelium). This explains why transitional cell carcinoma (TCC) can arise anywhere along this tract, and why a patient with bladder TCC must be surveilled for upper tract disease (and vice versa). This shared lining is called the “urothelial field” — a key MRCS concept linking ureteric, bladder, and upper tract pathology.