🔬 Renal Physiology
Urology Basic Sciences — Topic 3 of 13. Body fluids, GFR, tubular handling, RAAS, aldosterone, ADH, diuretics, and acid–base — with surgical and clinical context throughout.
💧 Body Fluids & Glomerular Filtration
The 60-40-20 Rule — Body Fluid Distribution
Total body water (TBW) is approximately 60% of body weight — about 42 L in a 70 kg adult. This percentage is highest in newborns and adult males, and lowest in adult females and in patients with large amounts of adipose tissue (fat is anhydrous).
Surgical Relevance — IV Fluid Choices
Understanding fluid compartments explains why different IV fluids distribute differently:
Normal saline / Hartmann’s (isotonic) → stays in ECF only. Does not shift water into or out of cells. Expands both plasma and interstitial compartments. Use: resuscitation, maintenance.
5% Dextrose (hypotonic after glucose metabolised) → distributes as free water across all compartments (⅔ goes intracellular). Risks hyponatraemia and cerebral oedema. Not a resuscitation fluid.
Hypertonic saline → pulls water from ICF into ECF. Used for severe hyponatraemia with neurological symptoms — cautiously (osmotic demyelination if corrected too fast).
Renal Blood Flow (RBF)
The kidneys receive approximately 25% of cardiac output — approximately 1.25 L/min in a 70 kg adult — despite accounting for only 0.5% of body weight. This enormous flow relative to metabolic need reflects the filtration function of the kidney, not oxygen demand.
Glomerular Filtration Rate (GFR)
Normal GFR is approximately 125 mL/min (180 L/day). Measured by inulin clearance — inulin is freely filtered, neither reabsorbed nor secreted. In clinical practice, GFR is estimated from serum creatinine (eGFR), though creatinine slightly overestimates GFR as it is secreted in small amounts by the proximal tubule.
Starling Forces at the Glomerulus
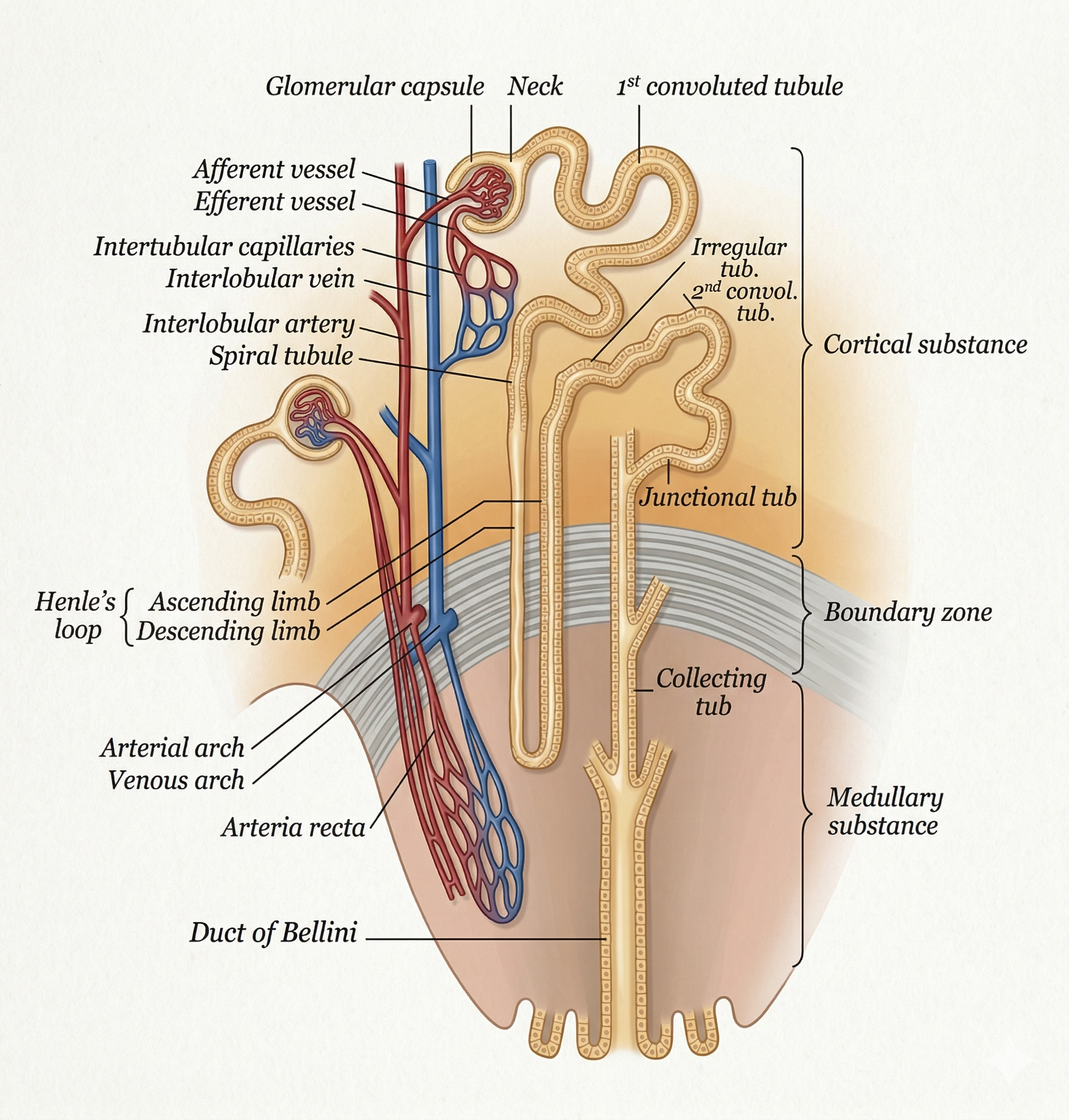
Glomerular filtration is driven by the balance of hydrostatic and oncotic pressures across the capillary wall. The diagram below shows the basic unit of the glomerulus with the afferent and efferent arterioles, Bowman’s capsule, and the direction of filtration forces.
ACE Inhibitors, ARBs & the Efferent Arteriole
Angiotensin II preferentially constricts the efferent arteriole, maintaining GFR when renal perfusion is reduced (e.g. renal artery stenosis, heart failure). ACE inhibitors and ARBs block this — they dilate the efferent arteriole, reduce PGC, and drop GFR. This is why ACE inhibitors are dangerous in bilateral renal artery stenosis or in a single functioning kidney. In practice: always check creatinine and potassium 1–2 weeks after starting ACE inhibitors. A rise in creatinine of up to 30% is acceptable; greater rises suggest renal artery stenosis. Long-term, ACE inhibitors protect the kidney in diabetic nephropathy by reducing hyperfiltration.
Autoregulation of RBF and GFR
Both RBF and GFR remain constant over a wide range of mean arterial pressure (80–200 mmHg) through two mechanisms:
- Myogenic mechanism: Increased pressure stretches afferent arteriole → reflex vasoconstriction → increased resistance → maintained flow.
- Tubuloglomerular feedback (TGF): ↑ GFR → ↑ NaCl delivery to macula densa → macula densa signals afferent arteriole to constrict → ↓ GFR back to normal. This couples filtration rate to tubular capacity.