🟡 Parathyroid Glands
Anatomy, embryology, PTH physiology, hyperparathyroidism (primary/secondary/tertiary), hypocalcaemia, surgical management — MRCS high-yield.
Anatomy & Embryology
Embryology
The parathyroid glands have a fascinating dual embryological origin from the 3rd and 4th pharyngeal pouches — and their origins are counterintuitively swapped compared to their final positions.
| Gland | Pharyngeal Pouch Origin | Travels With | Final Position |
|---|---|---|---|
| Superior parathyroids (P4) | 4th pharyngeal pouch | Thyroid gland (also from 4th pouch) | Posterior surface of thyroid, at junction of upper and middle thirds — consistent, predictable position |
| Inferior parathyroids (P3) | 3rd pharyngeal pouch — along with thymus | Thymus (descends further into chest) | Variable — near lower pole of thyroid, but can be anywhere from the angle of the jaw to the mediastinum, depending on how far the thymic descent carries them |
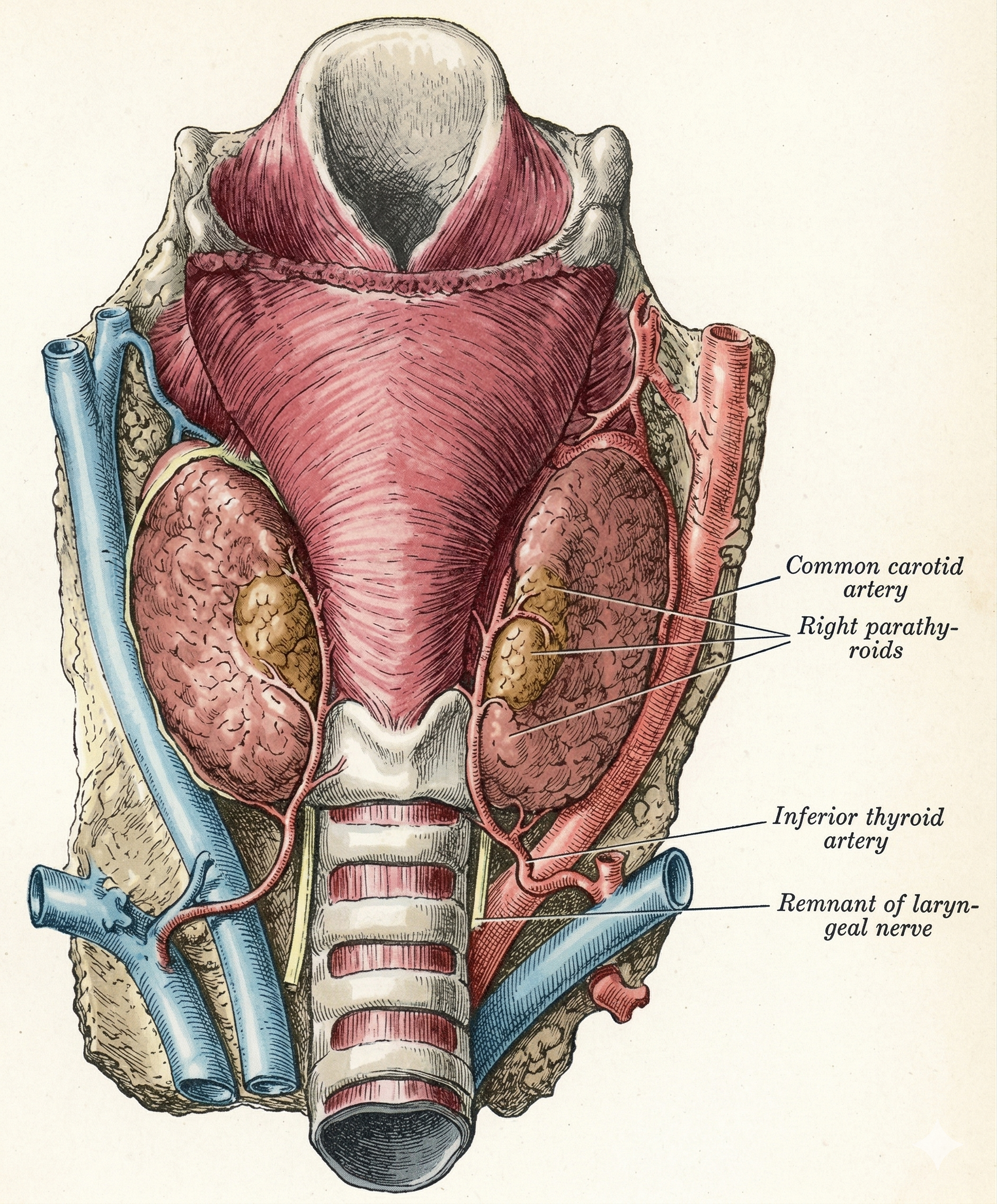
Parathyroid gland anatomy — positions of the superior (4th pouch) and inferior (3rd pouch) glands relative to the thyroid and surrounding structures.
The Pouch Paradox — “3 goes Lower, 4 stays Higher”
The counterintuitive fact: the inferior parathyroids come from the 3rd pouch (higher number = lower position seems backwards). The explanation: the 3rd pouch parathyroid travels with the thymus on its long descent toward the mediastinum — it descends past the 4th pouch parathyroid, ending up lower. The 4th pouch parathyroid travels only a short distance with the thyroid and stays superior.
This has surgical importance: inferior parathyroids are far more variable in position — they can lie anywhere from just below the lower thyroid pole to within the thymic fat pad in the anterior mediastinum. Missing an inferior gland in a re-operative neck (or failing to find one in primary hyperparathyroidism) often means looking in the mediastinum.
Gross Anatomy
| Feature | Detail |
|---|---|
| Number | Usually 4 (2 superior, 2 inferior). Supernumerary glands (~5th) present in ~5% — often within thymus or thyroid. Fewer than 4 present in ~3%. |
| Size / weight | ~5 × 3 × 1 mm; weight ~35–40 mg each. Appear as flat, oval, yellow-brown structures on the posterior thyroid surface. |
| Superior gland position | Consistent — posterior surface of thyroid, at the level where the inferior thyroid artery crosses the RLN (roughly junction of upper and middle thirds of the lobe) |
| Inferior gland position | Variable — most commonly near the lower thyroid pole or thyrotracheal groove. May be intrathyroidal (~1%), within thymic fat, retro-oesophageal, or in the posterior mediastinum. |
| Blood supply | Almost exclusively from the inferior thyroid artery (for both superior and inferior glands). This is why ligation of the inferior thyroid artery during thyroidectomy risks devascularising all parathyroids. |
| Identification | Distinguished from fat by their colour (browner than fat), lack of lobulation, and characteristic pattern of bleeding when nicked. Intraoperative PTH assay confirms function. |
Parathyroid Glands and the Inferior Thyroid Artery
The inferior thyroid artery is the dominant blood supply to the parathyroid glands. During thyroidectomy, the inferior thyroid artery should ideally be ligated distal to the parathyroid branches (close to the thyroid capsule) rather than ligated at its trunk — to preserve parathyroid vascularity. Mass ligation of the inferior thyroid artery trunk devascularises all four parathyroids simultaneously → permanent hypoparathyroidism. This is the same principle as ligating the superior thyroid artery close to the pole to protect the external laryngeal nerve.