🟣 The Appendix
Anatomy · Acute Appendicitis · Investigations & Scoring · Management · Wound Classification · Appendiceal Tumours · Surgical Technique — MRCS Part A & B
Anatomy of the Appendix
The vermiform appendix is a blind-ended true diverticulum of the colon — its wall contains all three layers (mucosa, submucosa, muscularis, serosa). It extends from the posteromedial aspect of the caecum, approximately 2.5 cm inferior to the ileocaecal valve.
The Appendix — Overview Diagram
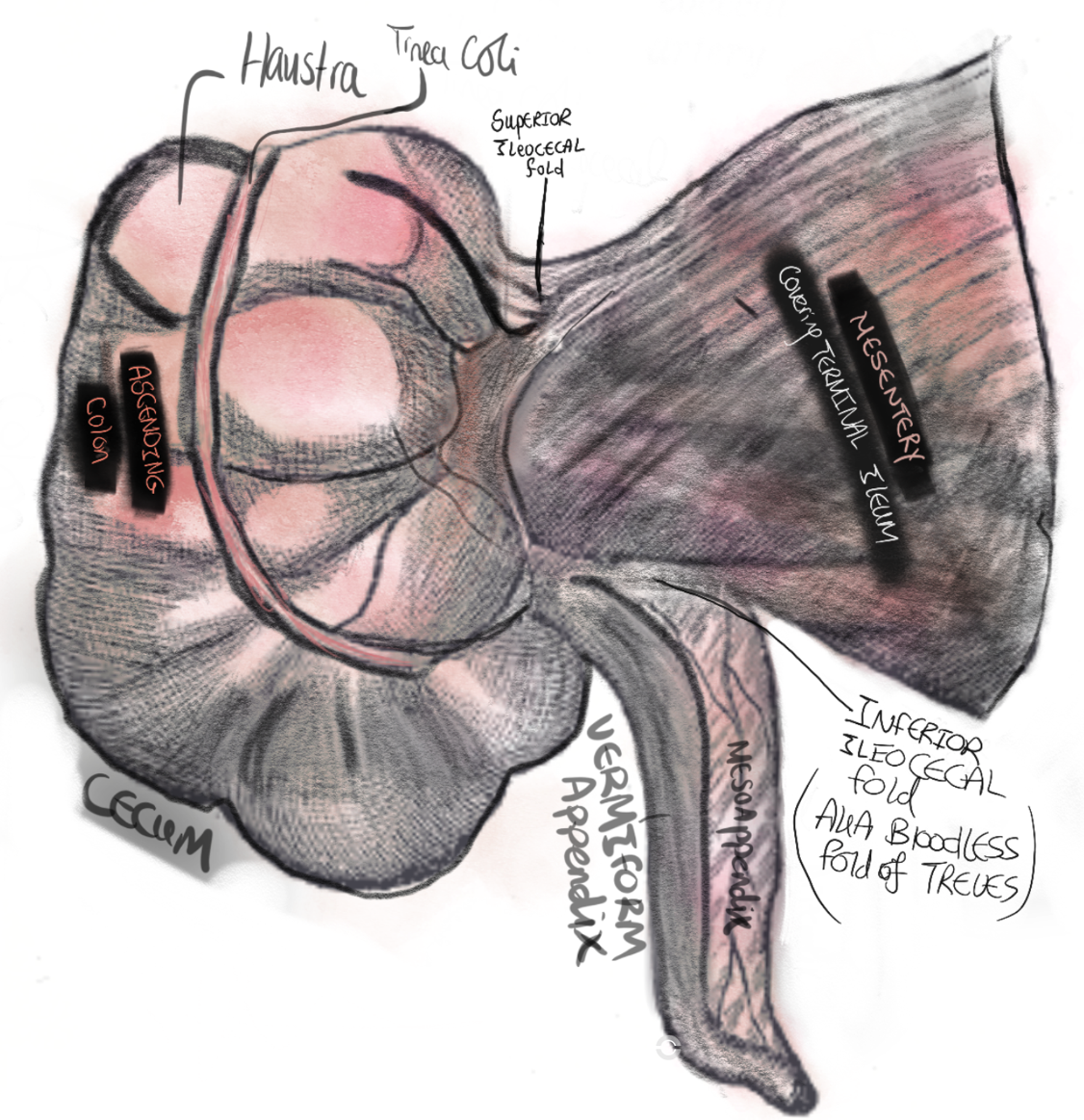
The appendix arises from the posteromedial caecum at the confluence of the three taeniae coli. The mesoappendix is a peritoneal fold containing the appendiceal artery (an end artery, branch of the ileocolic artery). The appendix has a complete outer longitudinal muscle layer — unlike the colon which has taeniae. Rich in submucosal lymphoid tissue (MALT).
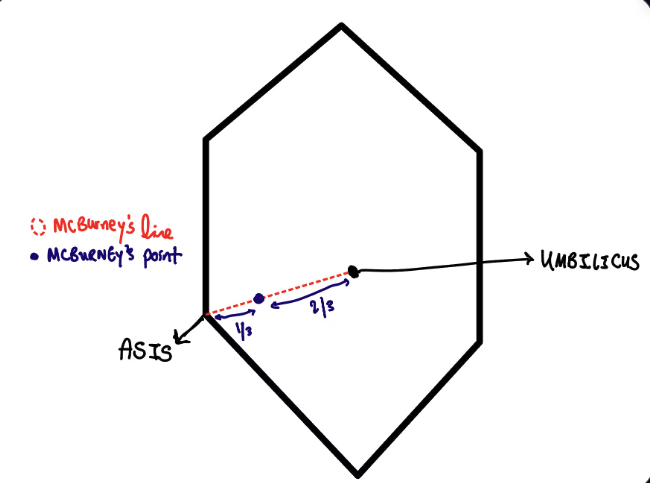
McBurney’s Point
Located at the junction of the lateral 1/3 and medial 2/3 of a line drawn from the right ASIS to the umbilicus. This is the surface marking for the appendiceal base, the site of maximal tenderness in appendicitis, and the centre of both the Gridiron and Lanz surgical incisions.
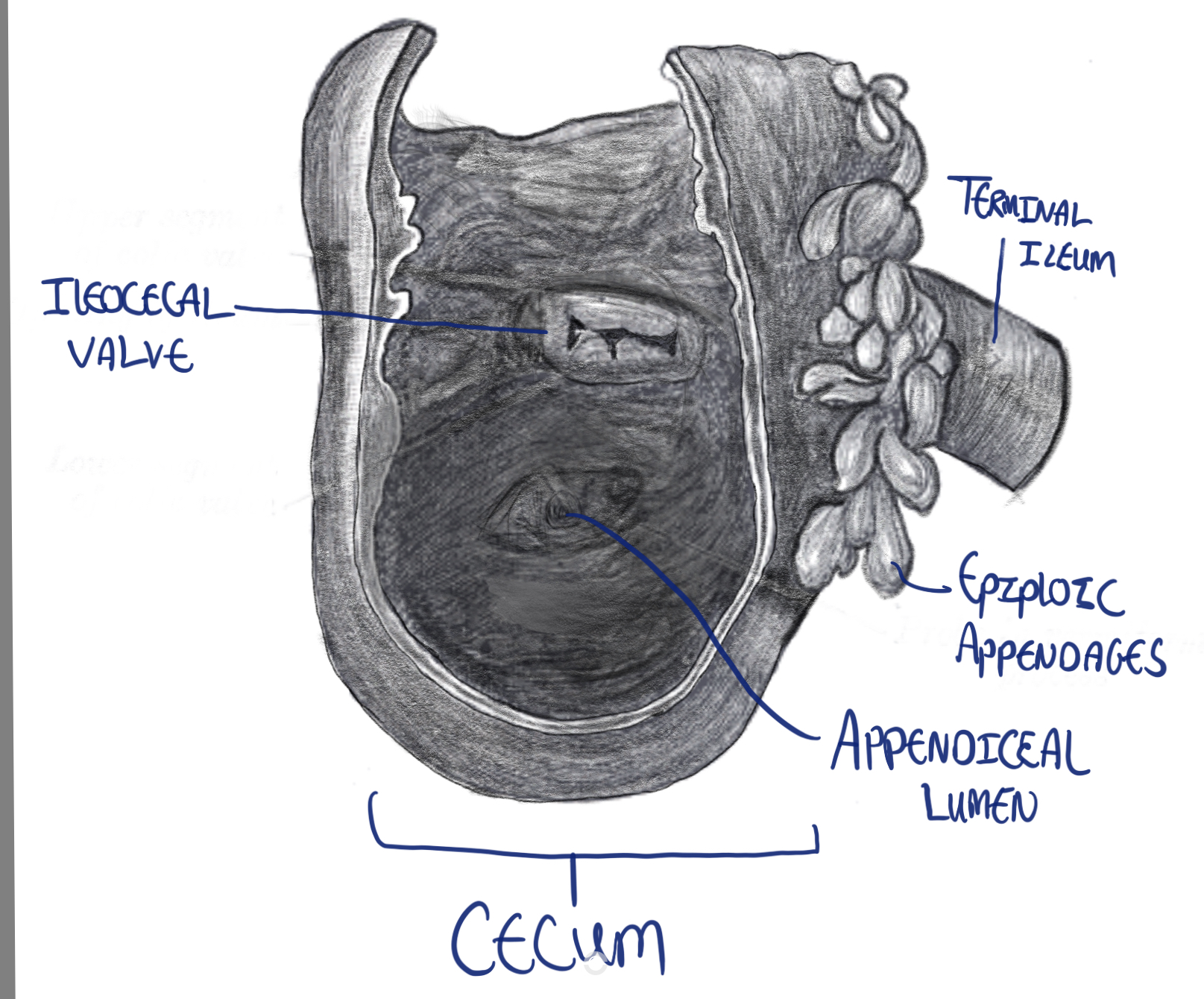
Appendix & Ileocaecal Valve
The appendiceal orifice opens into the caecal lumen approximately 2.5 cm inferior to the ileocaecal valve. The ileocaecal valve controls the passage of intestinal contents from the terminal ileum into the caecum and prevents reflux. The appendiceal base position is constant — only the tip position is variable.
McBurney’s Point — The Key Surface Landmark
The base of the appendix projects to McBurney’s point — at the junction of the lateral 1/3 and medial 2/3 of a line drawn from the right ASIS to the umbilicus. This is:
- The site of maximal tenderness in acute appendicitis (McBurney’s sign)
- The centre of both the Gridiron (McBurney’s) and Lanz open incisions
- The landmark for LIF laparoscopic port placement
How to Locate the Appendix Intraoperatively
The base is always constant — only the tip position varies. The reliable intraoperative method:
Follow the convergence of the three taeniae coli proximally along the ascending colon → they meet at the base of the caecum → this is exactly where the appendix arises.
This technique works in every position — retrocaecal, pelvic, or hidden by inflammation — because the taeniae always converge at the appendiceal base.
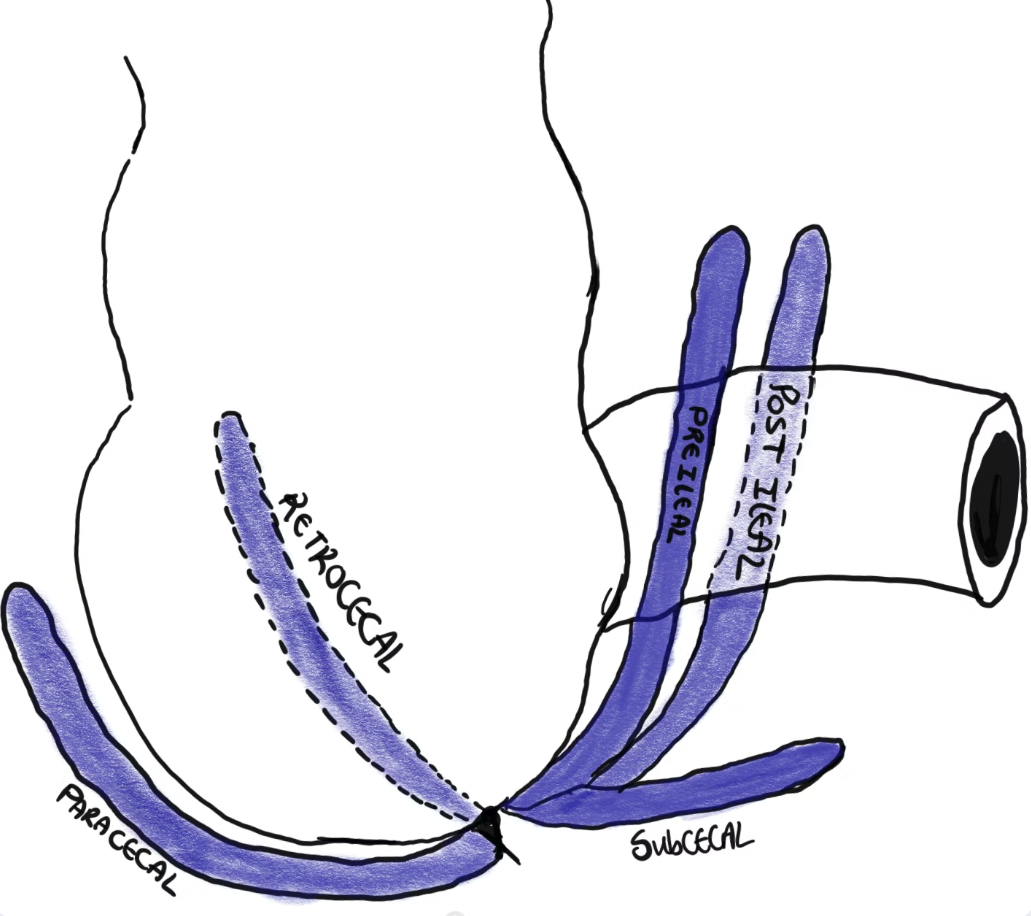
Variable Positions of the Appendix Tip
The base is fixed at the posteromedial caecum. The tip can lie in multiple positions — retrocaecal (65%, most common), subcaecal/pelvic (30%), preileal, postileal, or paracaecal. Each position produces a different clinical presentation, which explains the diverse and atypical presentations of appendicitis.
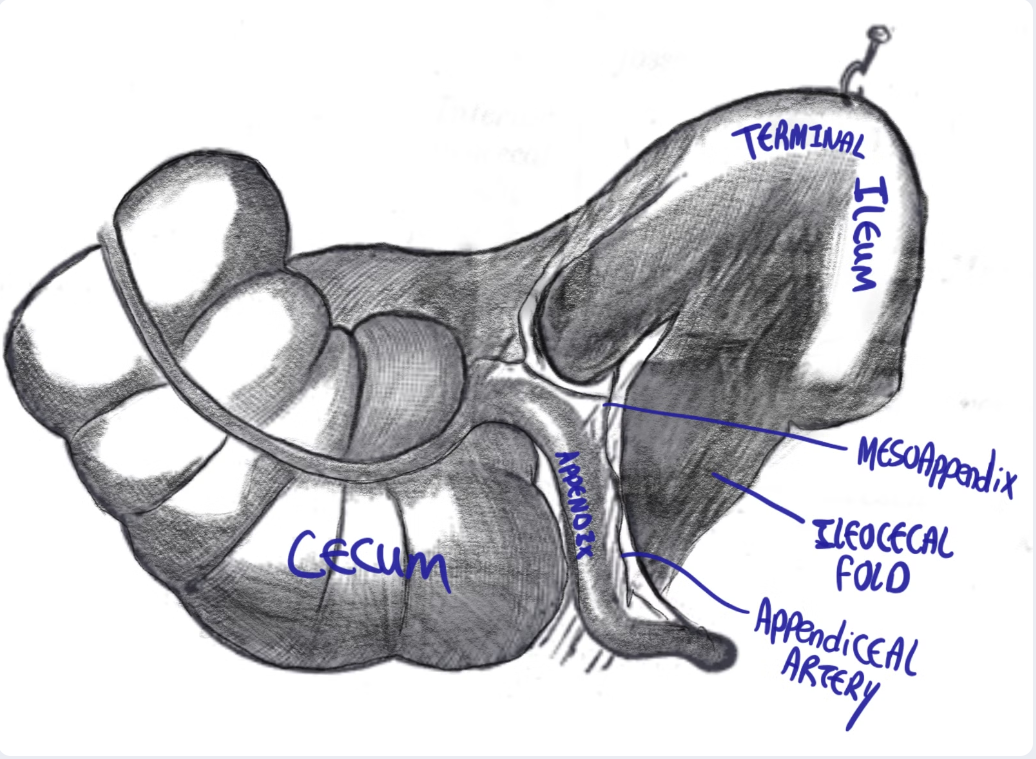
Mesoappendix & Bloodless Fold of Treves
The mesoappendix is a fold of peritoneum wrapping around the appendix, containing the appendiceal artery and vein. Its proximal attachment is the ileocaecal fold — the bloodless fold of Treves (named after Sir Frederick Treves who operated on King Edward VII, 1902). Despite the name, this fold frequently contains a small vessel and must be handled carefully.
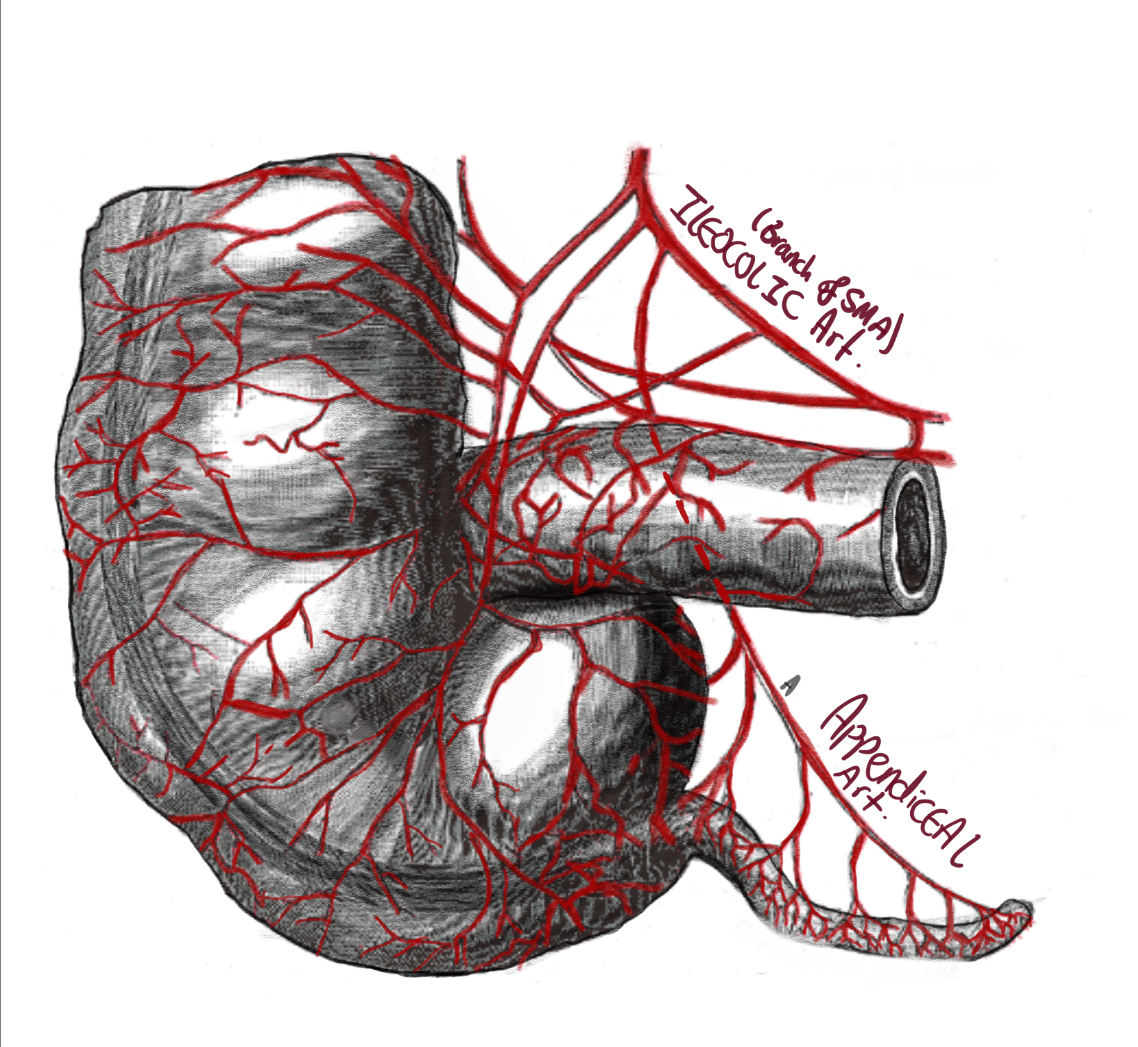
Appendiceal Arterial Supply
The appendiceal artery is a branch of the ileocolic artery (from the SMA). It runs in the free edge of the mesoappendix as an end artery with no collateral supply. In appendicitis, rising intraluminal pressure eventually occludes this single end artery → ischaemia → full-thickness necrosis → perforation. This explains why untreated appendicitis reliably progresses to gangrene and perforation.
- Artery
Appendiceal artery — branch of the ileocolic artery (SMA → aorta)
An end artery in the free edge of the mesoappendix. Sole supply with no collateral — rising intraluminal pressure in appendicitis → arterial occlusion → ischaemia → gangrene → perforation. Contrast: the gallbladder has a dual supply (cystic artery + liver bed) → perforation is less common.
- Vein
Appendiceal vein → ileocolic vein → superior mesenteric vein → portal vein → liver
Portal venous drainage — infective thrombus from appendicitis can track to the portal vein → pylephlebitis (septic portal vein thrombosis). Rare but life-threatening. Presents with spiking fevers, jaundice, and hepatic abscesses.
- Lymph
Nodes within the mesoappendix → ileocolic lymph nodes
Follows the vascular pedicle. Relevant in appendiceal tumour staging — ileocolic nodal involvement determines whether right hemicolectomy is required after appendicectomy.
- Nerve
Sympathetic afferents → T10 → periumbilical referred pain
T10 = umbilicus dermatome. Initial visceral pain in appendicitis is a dull periumbilical ache. Pain then migrates to the RIF as parietal peritoneum is irritated (somatic A-delta fibres → sharp, localised). This migration is the hallmark of appendicitis.
- True diverticulum — all three bowel wall layers present (mucosa, submucosa, muscularis, serosa)
- Rich in lymphoid tissue (MALT) — submucosal lymphoid follicles peak in adolescence, explaining peak incidence of appendicitis in young adults. Lymphoid hyperplasia is the most common cause of luminal obstruction in children/young adults.
- M cells (microfold cells) — sample and present antigens from the intestinal lumen to subepithelial lymphoid tissue
- Complete outer longitudinal muscle — unlike the colon, which has taeniae. The appendix has a regular, complete outer muscle layer.
- Lumen may be obliterated with age — progressive fibrosis obliterates the lumen → appendicitis becomes less common with advancing age as lumenal obstruction becomes impossible
- Taeniae coli — three 8 mm-wide longitudinal muscle bands on the colon wall. They converge at the appendiceal base (the basis for the intraoperative landmark). The appendix itself lacks taeniae.
| Measurement | Normal | Pathological Threshold |
|---|---|---|
| Length | Average 8–10 cm (range 2–20 cm) | Length alone is not indicative of pathology |
| Maximal Outer Diameter (MOD) | <6 mm | >6 mm = pathological |
| Maximal Mural Thickness (MMT) | <3 mm | >3 mm = pathological (target sign on CT) |