🟡 Gallbladder & Biliary System
Biliary anatomy · Bile physiology · Gallstone pathogenesis · Cholecystitis · Ascending cholangitis · ERCP · Laparoscopic cholecystectomy technique · PSC · Cholangiocarcinoma — MRCS Part A & B
Biliary Anatomy & Physiology
Bile is a physiological solution produced and secreted by hepatocytes at approximately 500–1000 mL/day. Its primary function is emulsification of dietary fat, vastly increasing the surface area available for pancreatic lipase. It also excretes cholesterol and bilirubin.
| Component | Function | Clinical Significance |
|---|---|---|
| Bile acids/salts (67%) | Amphipathic detergents — emulsify fat into micelles. Hydrophobic side binds fat; hydrophilic side faces the aqueous environment, keeping fat droplets separated and forming micelles for absorption at the terminal ileum. | Loss (Crohn’s, ileal resection) → reduced bile salt pool → cholesterol supersaturation → gallstone formation + secretory diarrhoea |
| Phospholipids (22%) | Lecithin — co-emulsifier. Keeps cholesterol solubilised in bile. | Imbalance → cholesterol precipitation → stone nucleation |
| Cholesterol (4%) | Eliminated via excretion as bile acid — maintains cholesterol homeostasis. | Supersaturation is the first step in cholesterol stone formation |
| Conjugated bilirubin | Waste product of haem metabolism — excreted in bile → stercobilin (faeces) and urobilinogen (urine). | Obstruction → conjugated hyperbilirubinaemia + pale stools + dark urine + pruritus |
| Water + Electrolytes | Solvent. Ductal cells (cholangiocytes) add bicarbonate (stimulated by secretin). | Biliary bicarbonate secretion = “bicarbonate umbrella” protecting ductal cells from acid |
After facilitating fat absorption, approximately 95% of bile acids are actively reabsorbed in the terminal ileum (via the ASBT transporter) → portal venous blood → liver → reconjugated and re-secreted. This recycling occurs 6–8 times daily, maintaining the bile acid pool without requiring full de novo synthesis.
Why Terminal Ileal Disease Causes Gallstones
Crohn’s disease, ileal resection, or radiation damage impairs active bile acid reabsorption → bile acid pool shrinks → bile becomes cholesterol-supersaturated → cholesterol stone formation. Bile acids reaching the colon cause secretory diarrhoea (bile acid malabsorption). This is why Crohn’s patients have dramatically higher gallstone rates.
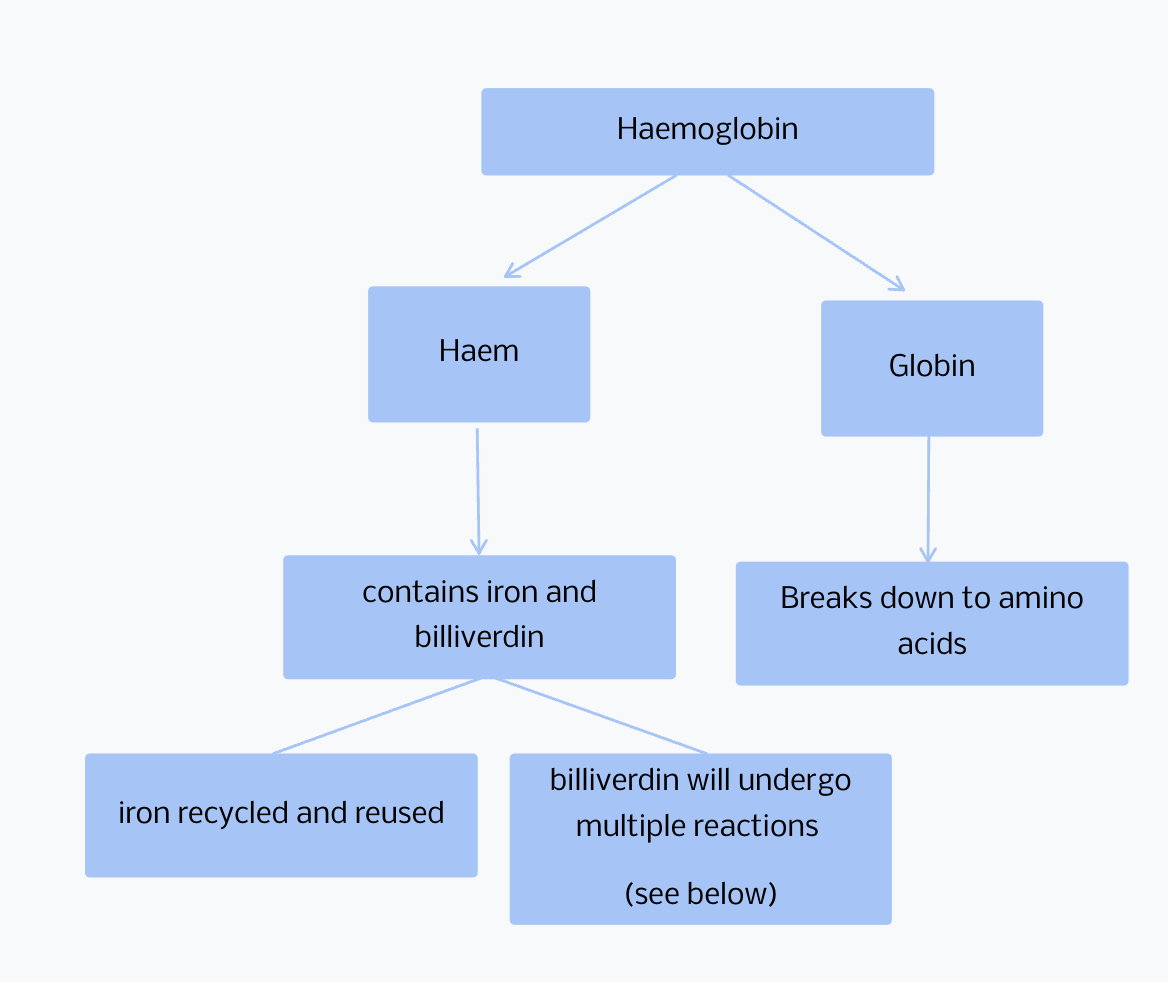
Haemoglobin → Biliverdin
Haem oxygenase cleaves the porphyrin ring of haemoglobin to yield biliverdin (green). This occurs in macrophages of the spleen, liver, and bone marrow.
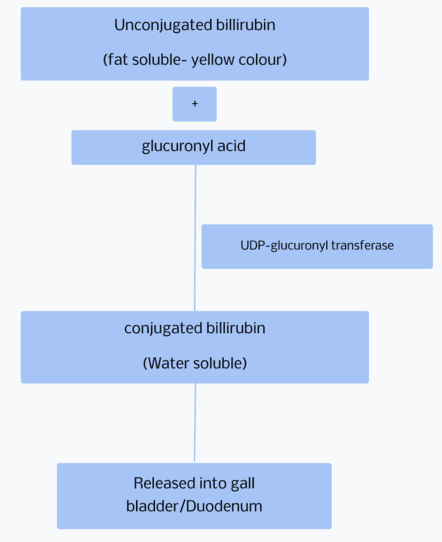
Biliverdin → Conjugated Bilirubin
Biliverdin reductase reduces biliverdin to unconjugated bilirubin. In hepatocytes, UGT1A1 (UDP-glucuronosyltransferase) conjugates bilirubin with glucuronic acid → water-soluble conjugated bilirubin → excreted into bile.
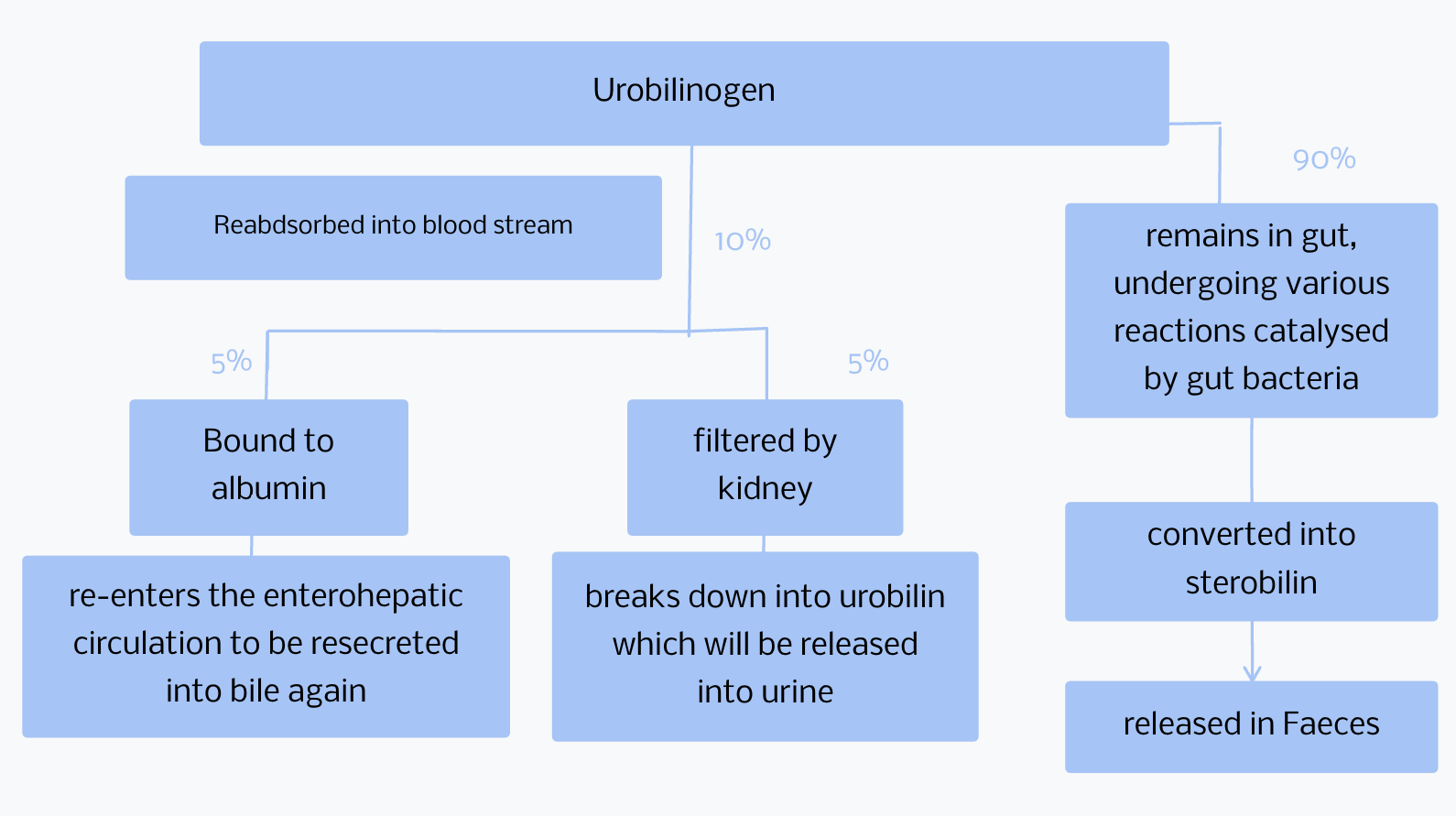
Urobilinogen → Stercobilin & Urobilin
Conjugated bilirubin in the intestinal lumen is deconjugated and reduced by gut bacteria to urobilinogen. Most is oxidised to stercobilin (brown stool pigment). A small amount is reabsorbed, re-excreted by the liver, or excreted in urine as urobilin (gives urine its yellow colour). In obstructive jaundice: no bilirubin reaches the gut → pale/clay-coloured stools + urobilinogen absent from urine.
Interpreting Jaundice — Pre-hepatic, Hepatic, or Post-hepatic?
Pre-hepatic (haemolytic): Unconjugated bilirubin overwhelms hepatic conjugation. Urobilinogen ↑ in urine, normal stool colour, NO conjugated bilirubin in urine. → Black pigment stones.
Hepatic (hepatocellular): Mixed picture — both fractions rise. ALT/AST markedly elevated.
Post-hepatic (obstructive): Conjugated bilirubin cannot reach gut → pale stools (no stercobilin), dark urine (conjugated bilirubin is water-soluble → spills into urine), pruritus (bile salt deposition). ALP and GGT markedly elevated. ALT only mildly elevated. NO urobilinogen in urine.
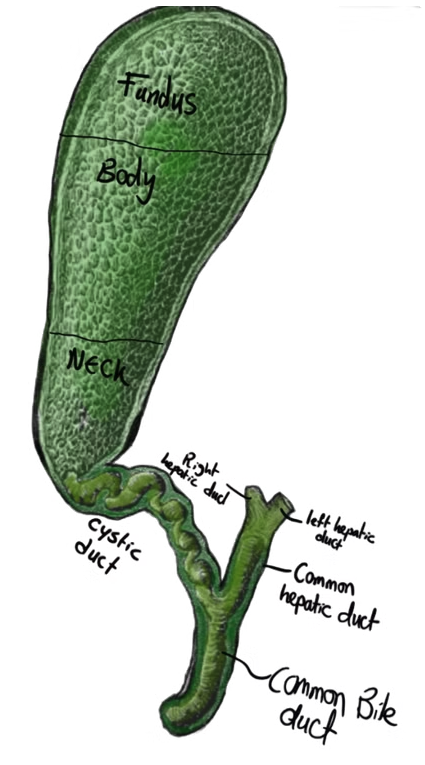
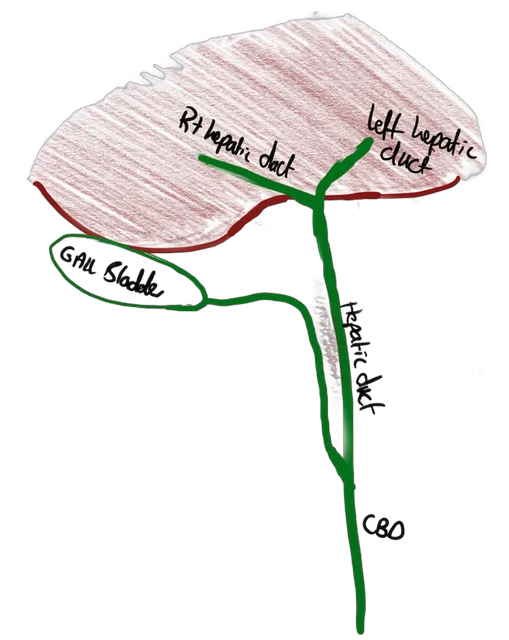
Gallbladder — Labelled Anatomy
The pear-shaped gallbladder sits in the gallbladder fossa on the visceral liver surface, right of the ligamentum teres. Capacity: 30–50 mL. Attached to the liver by loose fibro-areolar tissue. Sections: fundus (projects beyond liver edge) → body (overlies duodenum and transverse colon posteriorly) → neck (tapers to cystic duct; contains Hartmann’s pouch where stones most commonly lodge).
- F
Fundus
Projects beyond the inferior edge of the liver. The palpable part in a distended gallbladder (Courvoisier’s sign). Aligns with the right 9th costal cartilage tip.
- B
Body
Lies in contact with the liver bed (cystic plate). Posteriorly related to D1 duodenum and transverse colon — explains cholecystoduodenal fistula formation in recurrent cholecystitis.
- N
Neck + Hartmann’s Pouch
The neck tapers into the cystic duct. Hartmann’s pouch is the mucosal outpouching at the neck–body junction — the most common site for gallstones to lodge (biliary colic or cholecystitis). A stone here compressing the CHD = Mirizzi syndrome.
Microscopic Wall Structure (inside → out)
Mucosa (single layer of tall columnar epithelium + Rokitansky-Aschoff sinuses) → Lamina propria → Muscular layer (smooth muscle: circular, oblique, longitudinal) → Serosa (visceral peritoneum — covering the free inferior surface only; the hepatic surface has no peritoneum).
Relations
| Direction | Relation |
|---|---|
| Anteriorly / superiorly | Inferior edge of the liver |
| Posteriorly | Duodenum (D1) and transverse colon — risk of fistula formation |
| Inferiorly | Remainder of biliary tree + duodenum + transverse colon |
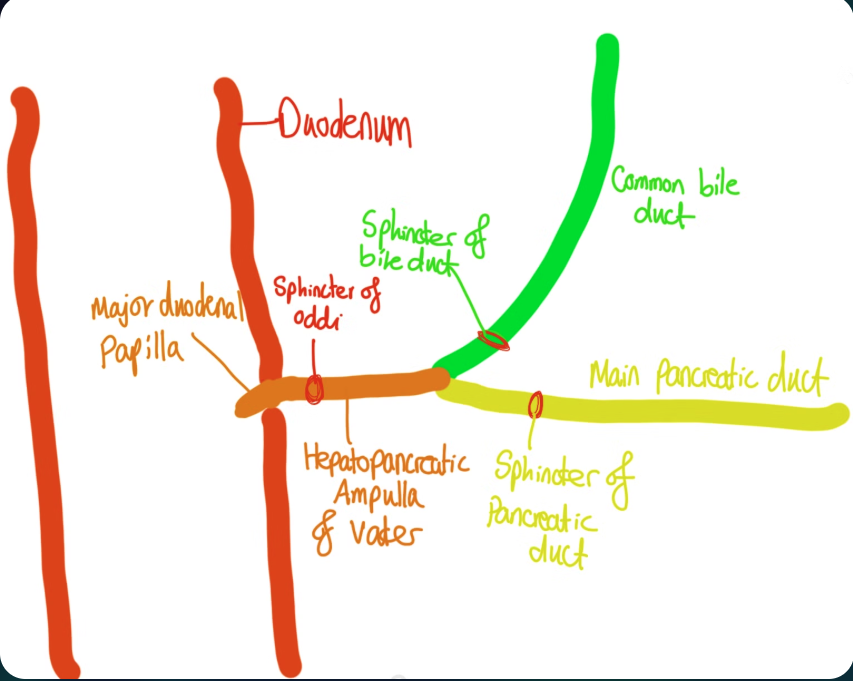
Distal Biliary Ducts & Sphincter Distribution — “Tube Map” Style
The CBD and main pancreatic duct converge to form the hepatopancreatic ampulla (ampulla of Vater), opening at the major duodenal papilla in D2 (~7 cm from the pylorus). The sphincter of Oddi surrounds the ampulla — contracts during fasting (bile diverted to gallbladder for storage/concentration), relaxes post-meal in response to CCK. In 85% of people the CBD and pancreatic duct share a common channel at the ampulla.
- 1
Bile canaliculi → Canals of Hering → Interlobular bile ducts
Hepatocytes secrete bile into canaliculi → Canals of Hering (lined by hepatocytes + cholangiocytes) → interlobular ducts running in portal triads with the portal vein and hepatic artery branches.
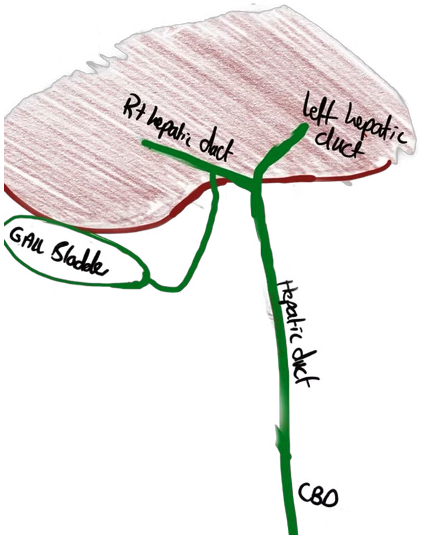
- 2
Right & Left Hepatic Ducts
Emerge at the porta hepatis. Right drains Couinaud segments V–VIII; left drains segments I–IV.
- 3
Common Hepatic Duct (CHD)
Right + left hepatic ducts unite at the porta hepatis. Length ~3–4 cm. Travels in the free edge of the lesser omentum.
- 4
Common Bile Duct (CBD)
CHD + cystic duct → CBD. Normal diameter ≤6 mm (up to 8 mm post-cholecystectomy or elderly). Spiral valve of Heister in the cystic duct. Three segments: supraduodenal (hepatoduodenal ligament) → retroduodenal (behind D1) → infraduodenal/intrapancreatic (embedded in pancreatic head → compressed by pancreatic carcinoma).
- 5
Ampulla of Vater + Sphincter of Oddi
CBD + main pancreatic duct (Wirsung) converge at the major duodenal papilla in D2. The sphincter of Oddi controls bile and pancreatic juice release — contracts during fasting, relaxes with CCK post-meal.
The hepatoduodenal ligament is the free edge of the lesser omentum. It contains the portal triad:
- CBD — right and anterior
- Hepatic artery proper — left and anterior
- Portal vein — posterior and central
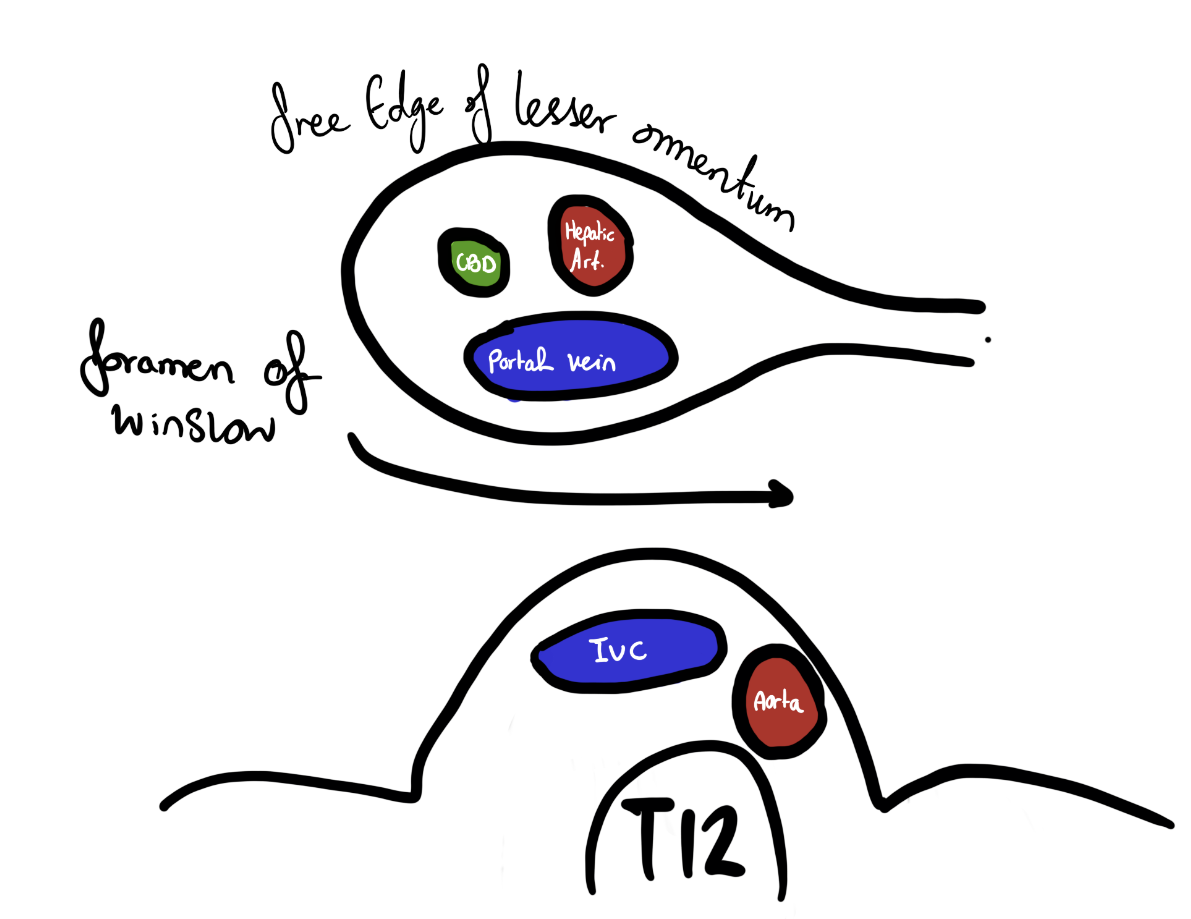
foramen of winslow and hepaticoduodenal ligament and structures involved in a pringle maneouver.
A portal triad of CBD (right and anterior), hepatic artery proper (left and anterior) and portal vein (posterior and central)
Pringle’s manoeuvre: compressing the hepatoduodenal ligament between the index finger (in the epiploic foramen) and thumb → simultaneously occludes all three structures → temporary arrest of hepatic inflow. Used during liver resection to control haemorrhage. The epiploic foramen (foramen of Winslow) lies immediately posterior to the hepatoduodenal ligament.
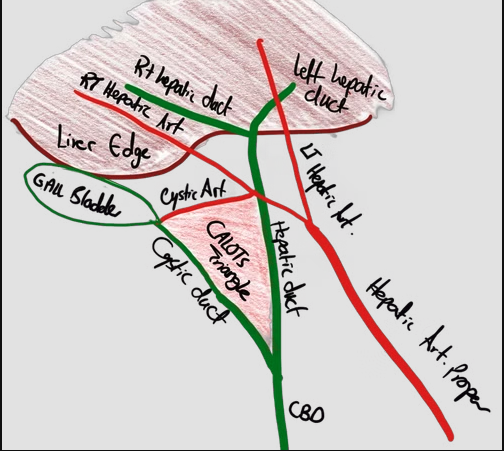
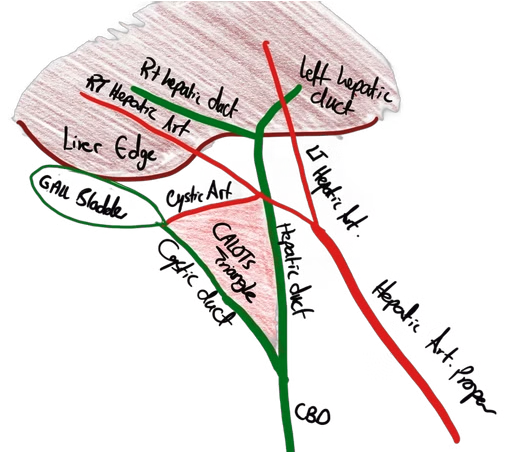
Calot’s Triangle (Original Description)
Borders: Superior — cystic artery · Lateral — cystic duct · Medial — hepatic duct.
Contents: Calot’s (Lund’s) lymph node. The original Calot’s triangle has the cystic artery as its superior border — this is the historical definition less used in modern surgery.
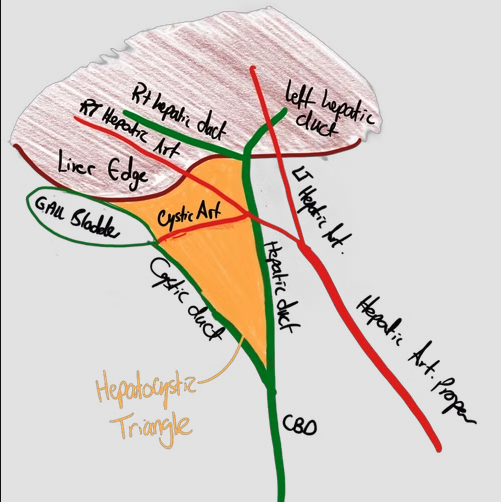
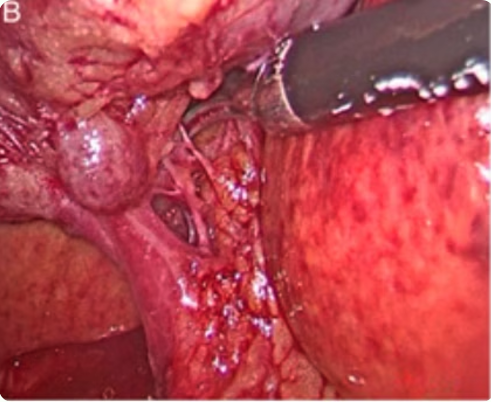
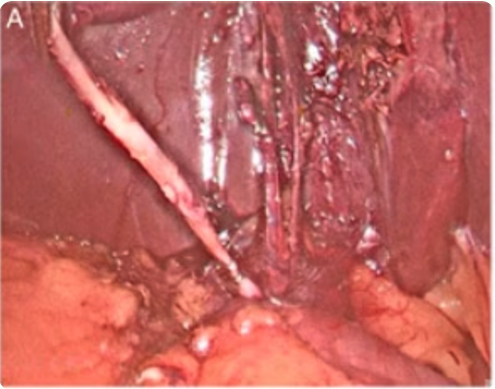
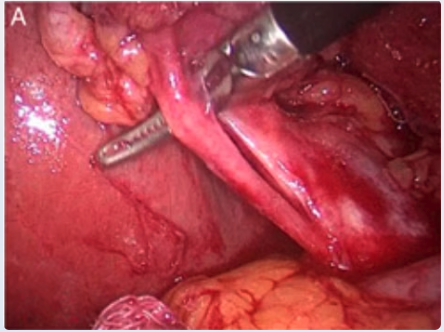
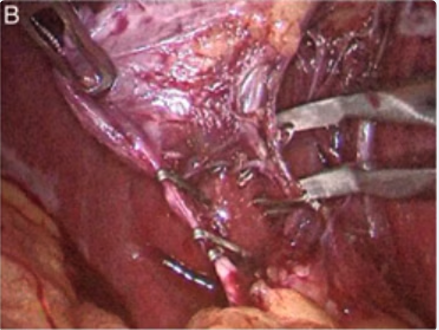
Hepatocystic Triangle (Modern Surgical Definition)
Borders: Superior — inferior edge of liver · Lateral — cystic duct · Medial — common hepatic duct.
Contents: Cystic artery (must be identified and clipped) + Calot’s/Lund’s node. The Critical View of Safety (CVS) must be achieved in this space before any clipping.
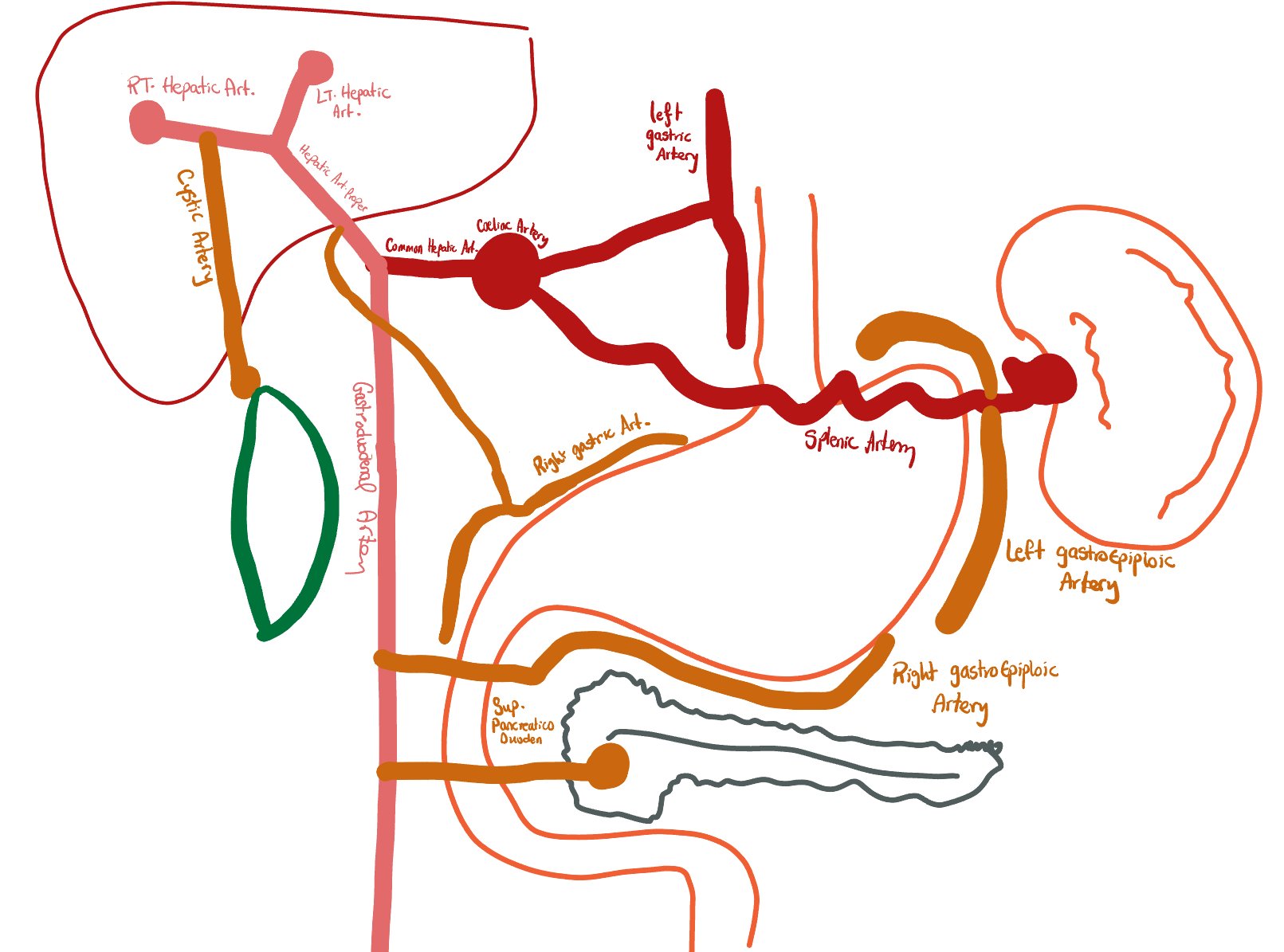
Cystic Artery Origin — Coeliac Axis “Metro Map”
The cystic artery normally arises from the right hepatic artery (→ hepatic artery proper → common hepatic artery → coeliac axis → aorta). The gallbladder also receives a secondary supply from the cystic plate of the liver. The cystic artery anatomy is highly variable — approximately 30% of patients have an anatomical variant. The most dangerous: the right hepatic artery forming a caterpillar hump (Moynihan’s hump) in the hepatocystic triangle, mimicking the cystic artery.
| Structure | Detail | Surgical Pearl |
|---|---|---|
| Cystic artery (main) | Branch of the right hepatic artery (RHA). Runs posterior to the cystic duct in the hepatocystic triangle. | Variable origin — may arise from left hepatic artery, GDA, main hepatic artery, or coeliac axis. Always confirm before clipping. |
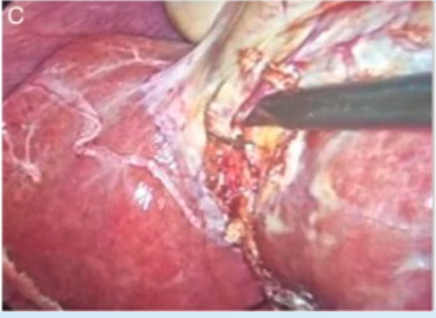
| Secondary supply | Direct arterial branches from the cystic plate (liver bed). | Explains why subtotal cholecystectomy can still leak bile from the liver bed (small Ducts of Luschka). |
| Lymphatics | Two chains: (1) between CBD and portal vein; (2) between hepatic artery and portal vein. First sentinel node = Calot’s/Lund’s node overlying the cystic artery insertion. | GB cancer lymphadenectomy requires skeletonisation of the CBD, portal vein, and hepatic artery with removal of all nodes above the duodenum. |
| Nerve supply | Sensory + sympathetic: coeliac plexus. Parasympathetic (motility): vagus (CN X). CCK stimulates contraction via vagal pathways. | Pain refers to right shoulder/scapula tip (phrenic nerve, C3-5). Explains right shoulder tip pain in biliary colic and cholecystitis. |
Approximately 30% of patients undergoing laparoscopic cholecystectomy have an anatomical variation. Misidentification is the leading cause of iatrogenic bile duct injury.
Gallbladder Variations
Normal Gallbladder
Standard position in the gallbladder fossa, right of the ligamentum teres.
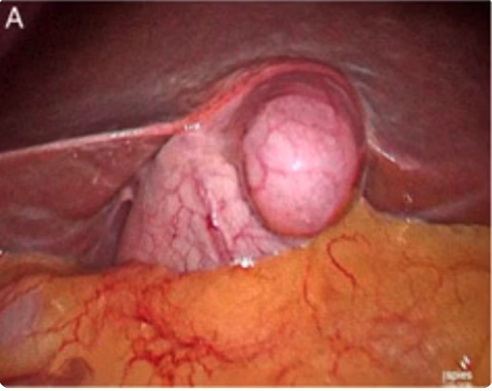
Gallbladder Diverticulum
Rare anomaly — a diverticular outpouching from the gallbladder wall. Can be mistaken for Hartmann’s pouch.

Intrahepatic Gallbladder
Entire circumference surrounded by liver parenchyma. Cholecystectomy risks major hepatic bleeding and bile leakage from ducts of Luschka.
Cystic Duct Variations
Normal Cystic Duct
Standard arrangement. The cystic artery (orange) lies posterior to the cystic duct, in the hepatocystic triangle. The normal cystic duct is 2–4 cm long.
Angular Insertion — 70% (Normal)
The cystic duct joins the CHD at a wide angle. The most common configuration. Easiest to dissect and clip safely.
Parallel Insertion — ~20%
Long cystic duct runs parallel alongside the CHD/CBD before joining. ⚠️ Can be mistaken for the CHD → inadvertent CBD clipping if not careful.
Spiral Cystic Duct — ~10%
The cystic duct spirals around the CHD before joining it. Can cross anteriorly. Extreme care needed to avoid CHD injury when clipping.
Long Cystic Duct (>4 cm)
Advantageous for manipulation and clipping — BUT a long spiralling duct is difficult to identify and increases the risk of CHD injury.
Cystic Duct → Right Hepatic Duct (Rare)
The cystic duct inserts directly into the right hepatic duct rather than the CHD. Division risks occluding the right hepatic duct → Strasberg type B ductal injury → right lobe infarction.
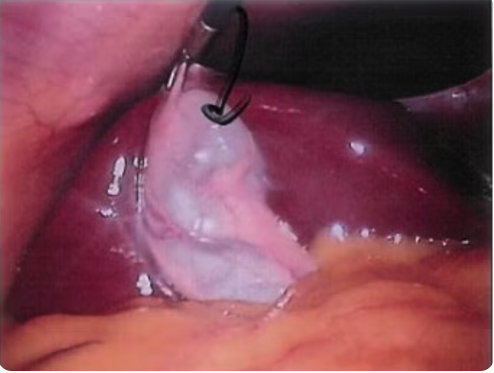
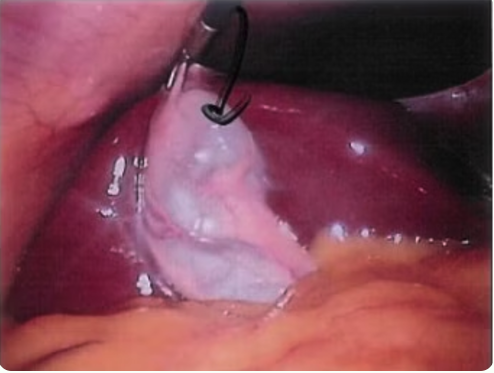
Cystic Artery Variations
Cystic Artery Anterior to Duct
If pulsation is not clearly visible, this vessel can be difficult to identify. ⚠️ May be confused with a fibrous band or missed entirely.
Double Cystic Artery (~15%)
⚠️ Can cause serious haemorrhage if only the first artery is clipped and the second is inadvertently divided without clips. Always check for a second artery before proceeding.
Cystic Artery from Liver Parenchyma
Arises directly from the liver parenchyma — no discrete pedicle available for clipping. Risk of liver bed haemorrhage. Requires diathermy or suture ligation.
Caterpillar Hump / Moynihan’s Hump
The right hepatic artery (or rarely the cystic artery) forms a loop (“caterpillar hump”) that bulges into the hepatocystic triangle. ⚠️ Misidentification and division of the right hepatic artery = devascularisation of the entire right lobe of the liver. Always confirm pulsation before clipping.
Cystic Artery Hump Variant
Another appearance of a tortuous or looped cystic artery variant. Always trace the vessel fully before applying any clips.
Double Cystic Duct
Rare anomaly. Two separate cystic ducts draining the gallbladder. Risk of incomplete clip occlusion and bile leak if the second duct is not identified and secured.