💪 Brachial Plexus Injuries
Erb’s “Waiter’s Tip” vs Klumpke’s “Claw Hand” — mechanisms, root levels, muscle losses, and the T1 avulsion → Horner’s syndrome boss-level trap.
The Brachial Plexus — Roots to Branches
The brachial plexus (C5–T1) supplies the entire upper limb. Trauma injuries split into two syndromes based on the direction of force: downward traction tears upper roots (Erb’s), upward traction tears lower roots (Klumpke’s). The plexus has five levels: Roots → Trunks → Divisions → Cords → Terminal branches.
| Root Level | Trunk | Key Functions | Injury |
|---|---|---|---|
| C5, C6 | Upper | Shoulder abduction (deltoid), elbow flexion (biceps), forearm supination | Erb’s palsy — Waiter’s Tip |
| C7 | Middle | Elbow extension (triceps), wrist/finger extension | Extended Erb’s (less common) |
| C8, T1 | Lower | Intrinsic hand muscles (lumbricals, interossei), wrist flexion | Klumpke’s palsy — Claw Hand |
| Type | Lesion Location | Surgical Repair? | Clinical Clue |
|---|---|---|---|
| Post-ganglionic (rupture) | Distal to dorsal root ganglion — in trunk, division, or cord | ✅ Yes — nerve graft or nerve transfer possible | Normal histamine flare test (axon reflex intact) |
| Pre-ganglionic (avulsion) | Root torn directly from spinal cord — worst injury | ❌ Cannot graft to spinal cord — nerve transfer only | Horner’s syndrome (if T1); MRI pseudomeningocele (CSF in dural tear) |
Pseudomeningocele on MRI = Pre-ganglionic Avulsion
When a root avulses, the dural sleeve tears. CSF tracks out and forms a fluid-filled outpouching at the nerve root level on MRI — a pseudomeningocele. This is the definitive radiological sign of a non-graftable pre-ganglionic injury and directly guides surgical planning.
Root Level Functional Memory
🔵 C5, C6 — Shoulder + Elbow flexion + Supination (Erb’s territory)
🟢 C7 — Elbow extension + Wrist/finger extension (middle territory)
🔴 C8, T1 — Intrinsic hand muscles + Wrist flexion (Klumpke’s territory)
Higher root = more proximal function. Lower root = more distal/fine function. The direction of the traction force determines which root group is stretched.
The brachial plexus is formed by the ventral rami of C5–T1. It passes from the intervertebral foramina through the posterior triangle of the neck, behind the clavicle, and into the axilla — changing its configuration at each anatomical level.
-
Roots
C5, C6, C7, C8, T1 — Ventral Rami
Emerge from the intervertebral foramina and pass between scalenus anterior (anteriorly) and scalenus medius (posteriorly) — the scalene triangle. The subclavian artery also passes through this triangle (important in thoracic outlet syndrome). Branches arising directly from the roots:
- Dorsal scapular nerve (C5) — rhomboids + levator scapulae
- Long thoracic nerve (C5, C6, C7) — serratus anterior. Injury → winged scapula
- Contribution to phrenic nerve (C5) — partial diaphragm innervation
-
Trunks
Upper (C5/C6), Middle (C7), Lower (C8/T1) — Posterior Triangle of Neck
Lie in the posterior triangle of the neck, superficial to scalenus medius. Pass over the first rib and beneath the clavicle. Interscalene block targets the upper trunk here. Branches:
- Suprascapular nerve (C5/C6) — upper trunk: supraspinatus + infraspinatus. Injury → weak abduction (0–15°) and external rotation
- Nerve to subclavius (C5/C6) — upper trunk: subclavius muscle
-
Divisions
Anterior (×3) + Posterior (×3) — Behind the Clavicle
Each trunk divides into anterior and posterior divisions behind the clavicle (retroclavicular space). The critical functional reorganisation:
- Anterior divisions → eventually supply flexor compartment muscles
- Posterior divisions → eventually supply extensor compartment muscles
- No named branches arise directly from the divisions — purely a reorganisation point
-
Cords
Lateral, Posterior, Medial — In the Axilla, Around the Axillary Artery
Named by their relationship to the second part of the axillary artery (behind pectoralis minor). Most anatomically complex level — multiple named branches arise here:
- Lateral cord (C5/6/7 anterior): lateral pectoral nerve → pec major; musculocutaneous nerve; lateral root of median nerve
- Posterior cord (all posterior divisions, C5–T1): upper + lower subscapular nerves → subscapularis + teres major; thoracodorsal nerve → latissimus dorsi; axillary nerve; radial nerve
- Medial cord (C8/T1 anterior): medial pectoral nerve → pec major + minor; medial cutaneous nerve of arm (C8/T1); medial cutaneous nerve of forearm (C8/T1); ulnar nerve; medial root of median nerve
-
Branches
Five Terminal Nerves — Musculocutaneous · Axillary · Median · Radial · Ulnar
- Musculocutaneous (C5/C6/C7 — lateral cord): pierces coracobrachialis → biceps + brachialis → continues as lateral cutaneous nerve of forearm
- Axillary (C5/C6 — posterior cord): quadrilateral space → deltoid + teres minor + regimental badge sensation. Injured in surgical neck of humerus fractures and anterior shoulder dislocation
- Median (C5–T1 — lateral + medial cords): formed by union of both roots in front of axillary artery → forearm flexors (except FCU), thenar muscles, lateral 2 lumbricals
- Radial (C5–T1 — posterior cord): winds in spiral groove of humerus → all extensors of elbow, wrist, fingers; brachioradialis. Mid-shaft humerus fracture → wrist drop (triceps spared — supplied above the groove)
- Ulnar (C8/T1 — medial cord): behind medial epicondyle → FCU, FDP (medial half), all interossei, medial 2 lumbricals, hypothenar muscles, adductor pollicis
| Nerve | Root | Cord | Motor Supply | Sensory | Reflex |
|---|---|---|---|---|---|
| Musculocutaneous | C5/C6/C7 | Lateral | Biceps, brachialis, coracobrachialis | Lateral forearm | Biceps jerk (C5/C6) |
| Axillary | C5/C6 | Posterior | Deltoid, teres minor | Regimental badge area (upper lateral arm) | — |
| Median | C5–T1 | Lateral + Medial | Forearm flexors (excl. FCU), thenar muscles, lat 2 lumbricals | Lateral 3½ digits (palmar) | — |
| Radial | C5–T1 | Posterior | Triceps, brachioradialis, all wrist + finger extensors | Posterior arm + forearm; dorsal lateral 3½ digits | Triceps jerk (C7); Brachioradialis jerk (C6) |
| Ulnar | C8/T1 | Medial | FCU, FDP (medial), all interossei, med 2 lumbricals, hypothenar, adductor pollicis | Medial 1½ digits (both surfaces) | — |
| Level | Location | Key Surgical Relations | Named Branches Arising |
|---|---|---|---|
| Roots | Between scalenus anterior and medius (scalene triangle) | Subclavian artery in the same triangle. Cervical rib compresses lower trunk here. Interscalene block risks phrenic nerve palsy (C5 root). | Dorsal scapular (C5), Long thoracic (C5/6/7), Phrenic contribution (C5) |
| Trunks | Posterior triangle of neck — above clavicle | Suprascapular vessels run alongside. Accessible for interscalene block (upper trunk). Clavicle fracture/callus can compress. | Suprascapular (upper trunk), Nerve to subclavius (upper trunk) |
| Divisions | Retroclavicular — behind the clavicle | Clavicular fractures can injure at this level. No regional block targets divisions specifically. | None |
| Cords | Axilla — around 2nd part of axillary artery, behind pec minor | Infraclavicular block targets cords. Axillary artery landmark. Pec minor retracted to expose cords in dissection. | Pectoral nerves, thoracodorsal, subscapular nerves, medial cutaneous nerves of arm + forearm |
| Branches | Axilla and upper arm — distal to pec minor | Axillary block targets branches in the axilla. Axillary nerve at risk in shoulder dislocation + surgical neck fractures. Radial nerve in spiral groove with mid-shaft humeral fractures. | Five terminal nerves |
The Median Nerve — Two Roots from Two Cords
The median nerve is unique in receiving contributions from both the lateral cord (C5/6/7) and the medial cord (C8/T1). The two roots unite in front of the axillary artery. This means median nerve function is affected in both:
🔵 Upper plexus injuries (lateral root loss → loss of lateral cord C5/6/7 contribution → thenar weakness, pronation weakness)
🔵 Lower plexus injuries (medial root loss → C8/T1 → thenar and lumbrical loss in Klumpke’s)
The median nerve is the plexus “bridge” — its two-cord origin is the anatomical reason it has such a wide territory and is the most functionally complex nerve in the upper limb.
Thoracic Outlet Syndrome — Compression at Root/Trunk Level
Thoracic outlet syndrome (TOS) occurs when the neurovascular bundle is compressed in one of three spaces: the scalene triangle, between the clavicle and first rib, or between pec minor and the ribs. Three types:
🔴 Neurogenic TOS (~95%) — lower trunk (C8/T1) most commonly compressed → medial forearm and hand symptoms, intrinsic hand muscle wasting. Causes: cervical rib, anomalous first rib, scalene hypertrophy, fibrous band from C7 transverse process
🟡 Venous TOS — subclavian vein compression → upper limb DVT (Paget-Schroetter syndrome — effort thrombosis in young athletes)
🟡 Arterial TOS — subclavian artery compression → hand ischaemia, Raynaud’s. Risk of distal thromboembolism — most dangerous type
Cervical rib (rudimentary C7 rib, present in ~0.5% of population) is the most common predisposing anatomical anomaly. Diagnosed on CXR/CT. Treatment: physiotherapy first; surgical first rib ± cervical rib resection via transaxillary or supraclavicular approach for refractory cases.
Reference diagrams showing the five levels of the brachial plexus — from roots (C5–T1) through trunks, divisions, and cords to the terminal peripheral nerve branches.
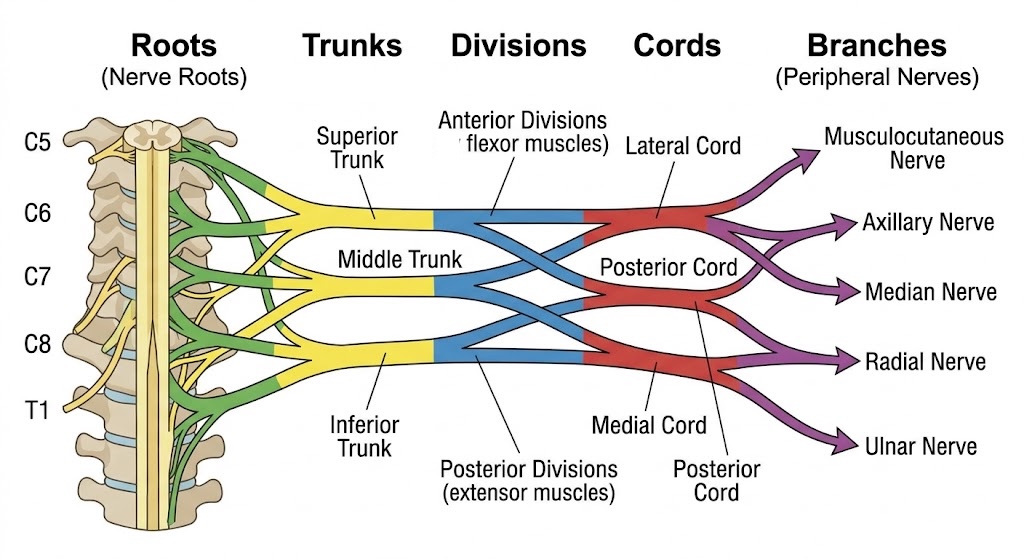
Roots → Trunks → Divisions → Cords → Branches
Colour-coded anatomical diagram. Anterior divisions (yellow) → flexor muscles via lateral and medial cords. Posterior divisions (blue) → extensor muscles via posterior cord. Terminal branches: musculocutaneous, axillary, median, radial, ulnar.
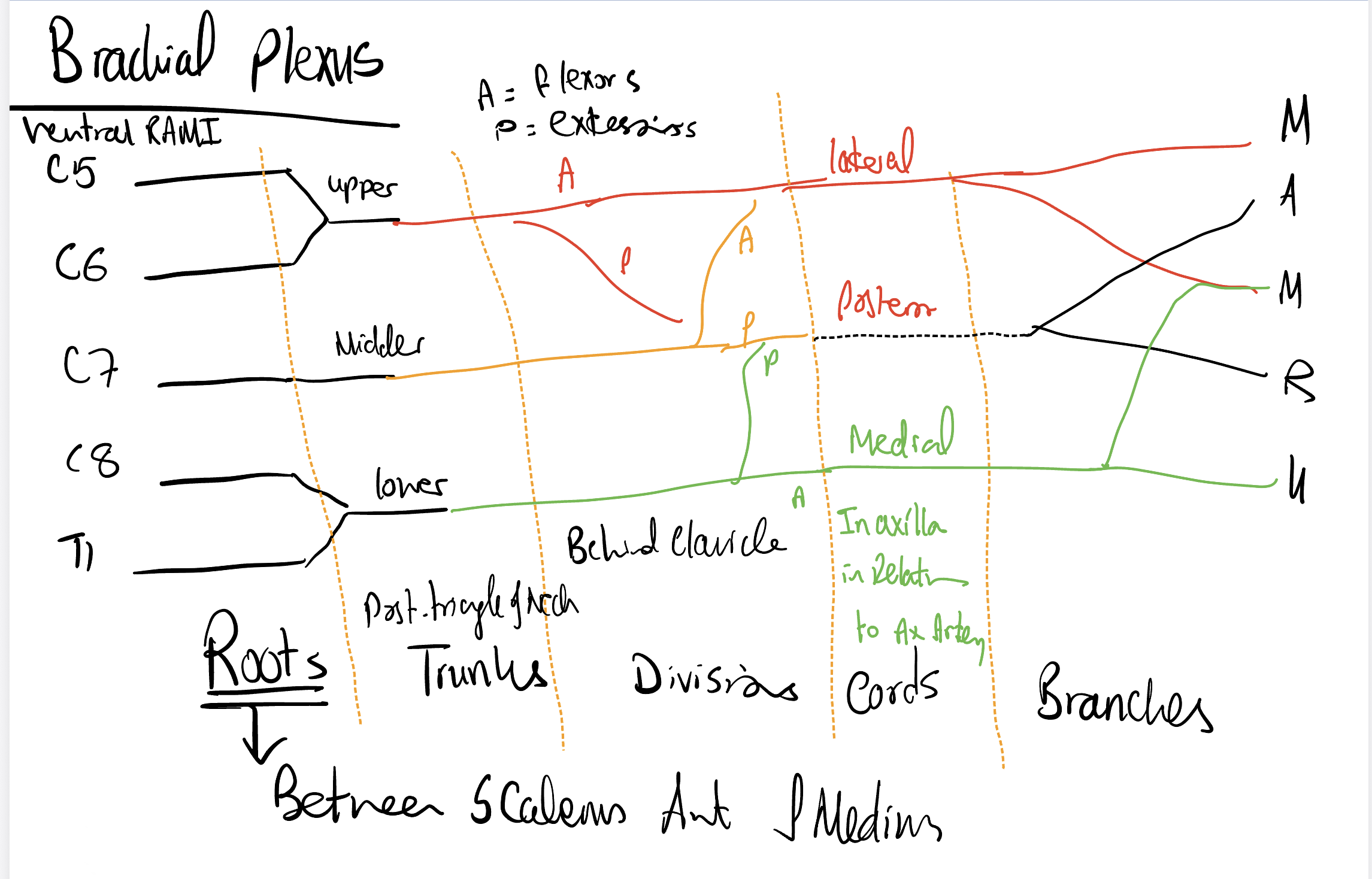
Annotated Schematic — Roots between Scalenes
Hand-drawn schematic showing anatomical locations: roots between scalenus anterior and medius, trunks in the posterior triangle of the neck, divisions behind the clavicle, cords in the axilla in relation to the axillary artery. A = anterior (flexors); P = posterior (extensors). M = musculocutaneous, A = axillary, M = median, R = radial, U = ulnar.