🟤 The Liver
Liver anatomy and Couinaud segmentation, clinical assessment, jaundice, portal hypertension and varices, cirrhosis and its complications, and hepatic masses.
Liver Anatomy
The liver is the largest internal organ and gland in the body, weighing approximately 1.5 kg in adults. It sits in the right upper quadrant directly beneath the diaphragm, with its normal span less than 12.5 cm on percussion in the mid-clavicular line. A tongue-like projection from the right lobe’s inferior surface known as Riedel’s lobe is an anatomical variant that can be mistaken for hepatomegaly or a right-sided mass.
| Surface | Description | Key Features |
|---|---|---|
| Diaphragmatic surface | Smooth, convex, dome-shaped — moulds against the concavity of the diaphragm. Covered by visceral peritoneum except posteriorly. | Bare area — a postero-superior region directly in contact with the diaphragm and right adrenal gland. No peritoneum here. Bordered by reflections of the coronary and triangular ligaments. Provides a direct route for right-sided pleural effusion ↔ hepatic pathology. |
| Visceral surface | Concave postero-inferior surface bearing impressions of adjacent organs. Separated from diaphragmatic surface by the sharp inferior border. | Right lobe: renal, duodenal, and colic impressions. Left lobe: gastric impression + oesophageal groove. Gallbladder fossa on the infero-anterior surface. The H-shaped fissures and porta hepatis are on this surface. |
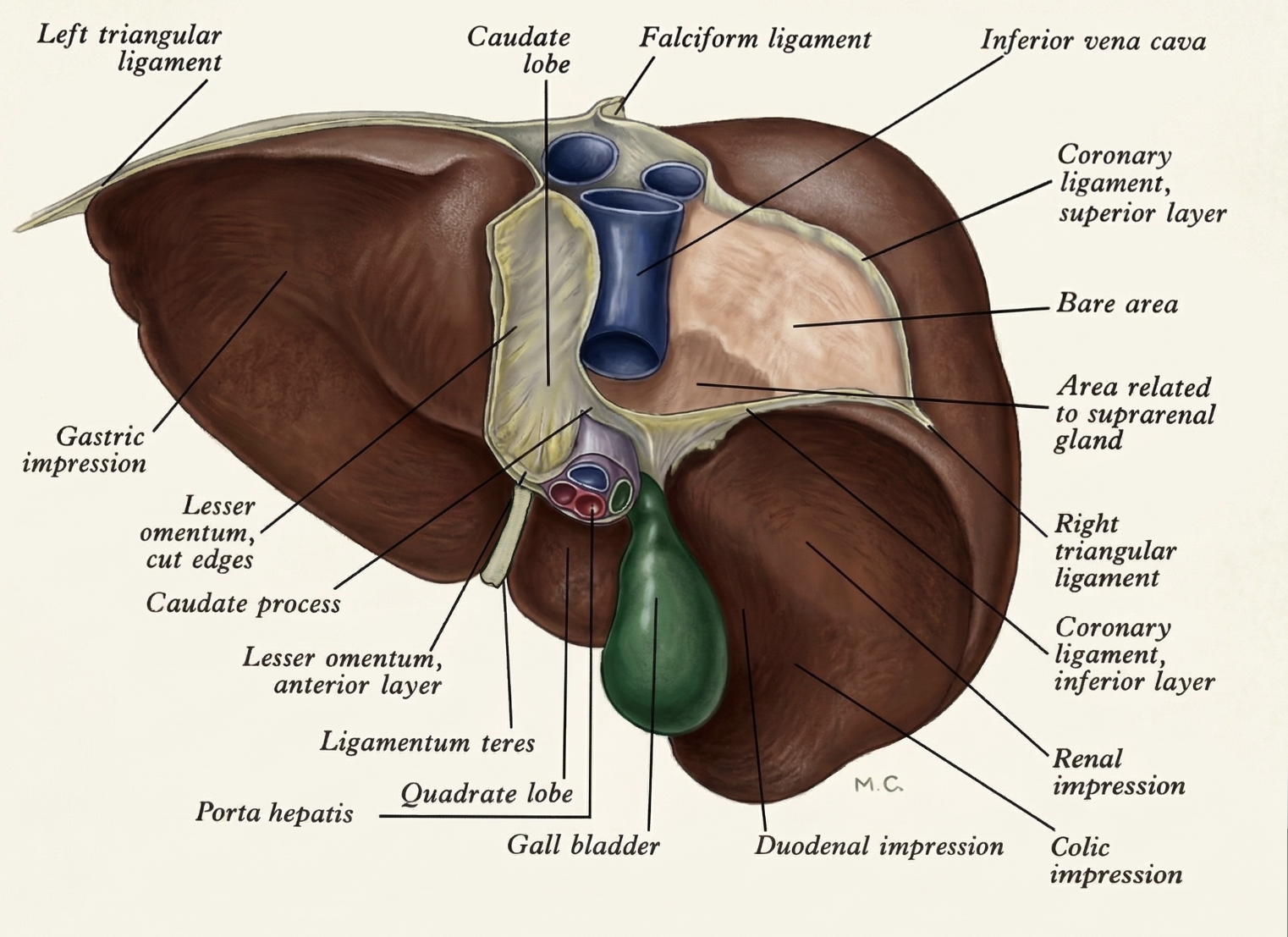
The posterior aspect of the liver showing the bare area, coronary ligaments, and posterior relations
The posterior surface of the liver is the region most closely related to the diaphragm, IVC, and retroperitoneal structures. Key landmarks visible from this view include:
- Bare area of the liver — a large, roughly triangular area on the postero-superior surface that is not covered by peritoneum. It is directly in contact with the diaphragm, separated only by areolar connective tissue. Bounded superiorly and inferiorly by the upper and lower layers of the coronary ligament, and laterally by the right triangular ligament.
- Coronary ligament — the peritoneal fold that reflects from the diaphragm onto the liver, defining the upper and lower borders of the bare area. The upper and lower leaves of the coronary ligament meet laterally to form the right triangular ligament.
- Left triangular ligament — attaches the left lobe of the liver to the diaphragm. Can be divided during left-sided hepatic surgery.
- Retrohepatic IVC — runs in its groove along the posterior surface, receiving the three main hepatic veins (right, middle, left) and the short hepatic veins from the caudate lobe just below the diaphragm.
- Right adrenal (suprarenal) gland impression — sits directly in the bare area, directly adherent to the posterior liver surface. This is why right adrenalectomy can be a challenging dissection.
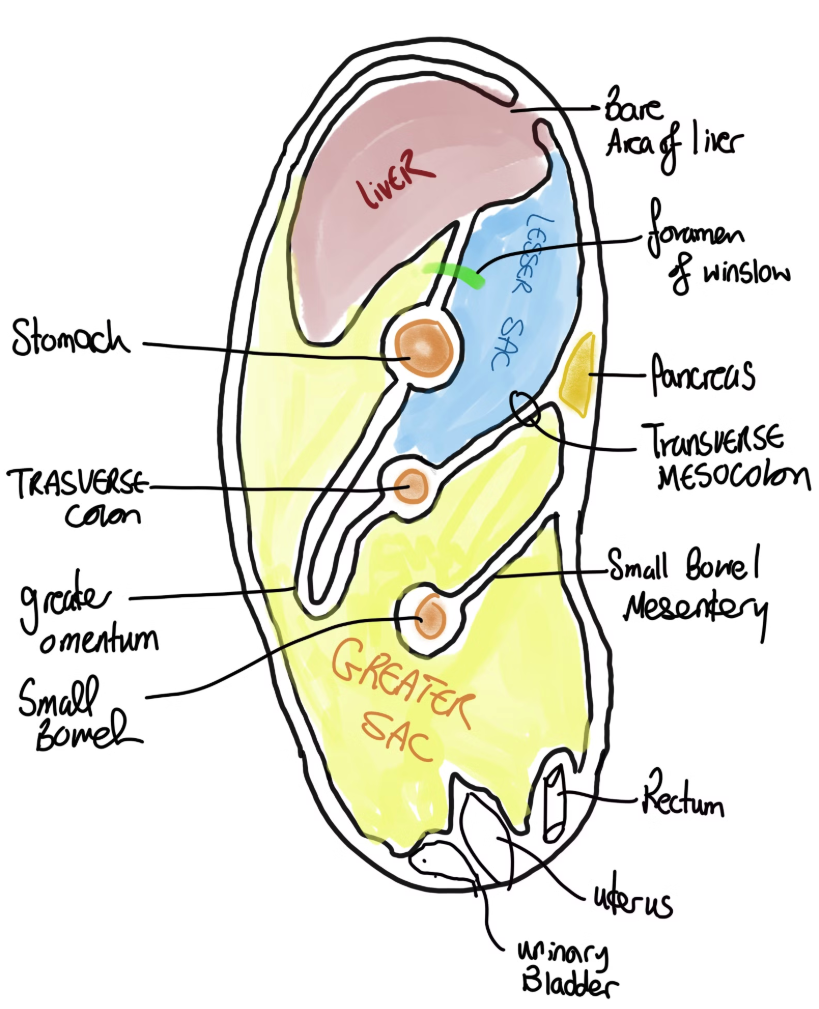
Sagittal view showing the peritoneal reflections, the bare area of the liver in contact with the diaphragm, and the relationship to the lesser sac
The bare area is clinically important because it is the only region of the liver surface that lacks a peritoneal covering, placing it in direct contact with the diaphragm and the retroperitoneum. This has important consequences:
- Direct communication between the hepatic and pleural spaces: The bare area is separated from the right pleural cavity only by the diaphragm. Lymphatics from the liver traverse the diaphragm here, creating a pathway between the hepatic parenchyma and the right pleural space. This explains why large right liver lesions, hepatic abscesses, or traumatic haematomas can track superiorly to cause a right-sided sympathetic or reactive pleural effusion — without needing to pass through the peritoneal cavity.
- Clinical relevance in infections and abscesses: A pyogenic hepatic abscess (most commonly in the right lobe — the terminal branch of the portal vein preferentially directs septic emboli into the right liver) can rupture through the bare area into the right pleural cavity, causing an empyema thoracis, or track through the diaphragm into the pericardium (rare but potentially fatal). In amoebic liver abscess (Entamoeba histolytica), right lobe abscesses can rupture through the bare area directly into the right lower pleural space — the most common complication of amoebic liver abscess. This occurs without peritoneal soiling because the bare area bypasses the peritoneal cavity entirely. Clinically: right lobe hepatic abscess + new right pleural effusion on CXR = suspect transphrenic spread through the bare area until proven otherwise.
- Hepatic hydrothorax — in cirrhosis with massive ascites, ascitic fluid can transude through small diaphragmatic defects in the bare area region into the right pleural space, causing a right-sided hepatic hydrothorax even with relatively little abdominal ascites visible.
- Surgical relevance: During hepatic mobilisation, the bare area must be carefully dissected off the diaphragm. Uncontrolled entry into the right pleural cavity during this manoeuvre requires immediate recognition and closure.
Bare Area — Why Right-Sided Liver Disease Causes Pleural Effusions
The bare area’s direct contact with the diaphragm creates a lymphatic highway between the liver and the right pleural space. In any condition that increases hepatic lymphatic flow (portal hypertension, hepatic congestion, malignancy, abscess), this pathway becomes overwhelmed and lymphatic fluid transudates into the right pleural space.
Key clinical scenarios:
🔵 Pyogenic hepatic abscess (right lobe) → can rupture via bare area → right empyema or pericarditis
🔵 Amoebic liver abscess → most common complication is right pleural rupture through bare area
🔵 Hepatic hydrothorax in cirrhosis → ascitic fluid passes through diaphragmatic defects in bare area → right pleural effusion
🔵 Right subphrenic abscess → can spread via bare area to right pleural cavity
🔵 Hepatocellular carcinoma → direct diaphragmatic invasion possible via bare area
A right-sided pleural effusion in any patient with known liver disease or right upper quadrant pathology should always prompt consideration of a hepatic origin via the bare area.
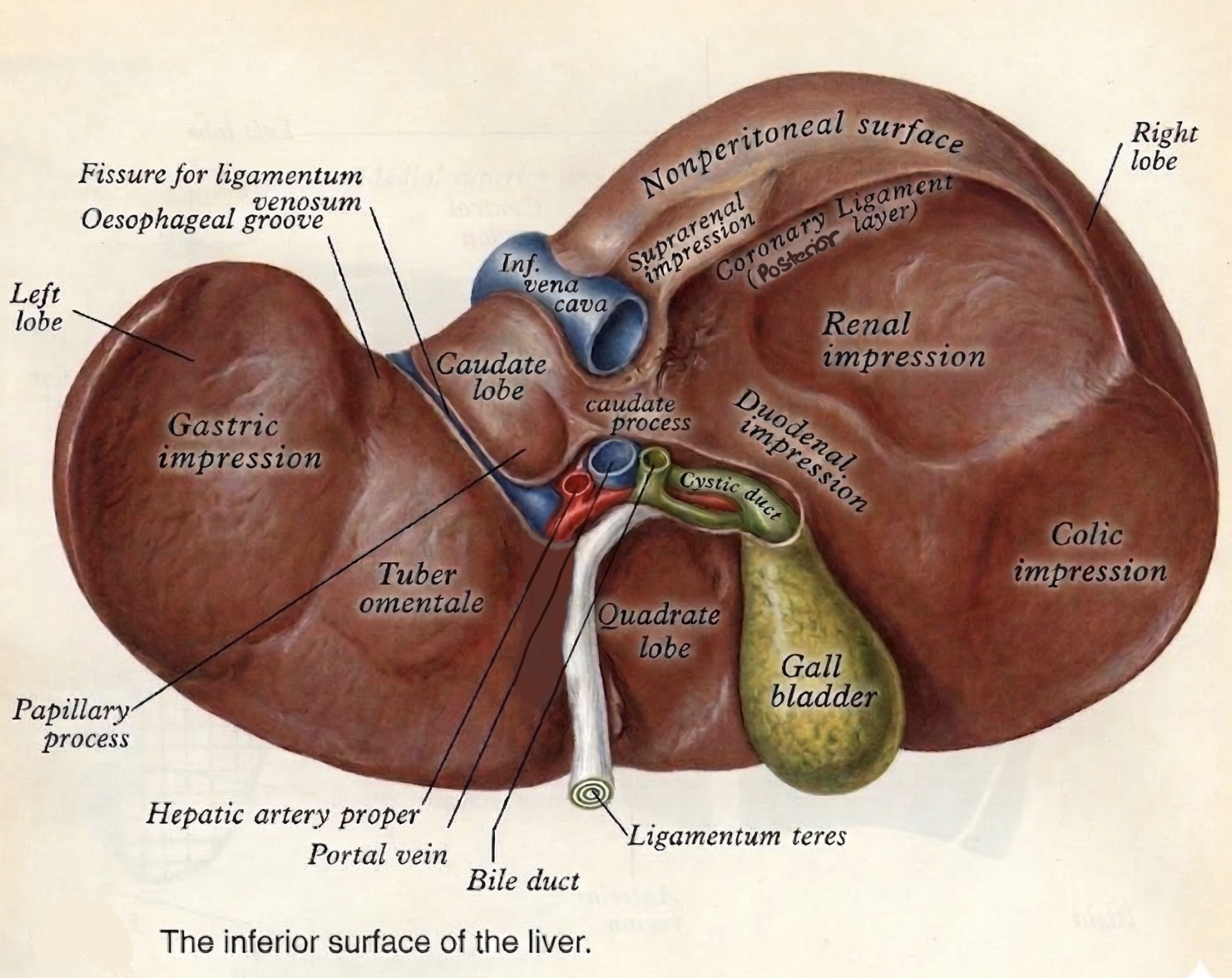
The inferior (visceral) surface of the liver showing the H-shaped fissures, porta hepatis, gallbladder fossa, and organ impressions
The visceral (inferior) surface faces downward and posteriorly, bearing the H-shaped pattern of fissures and fossae that divides it into four traditional lobes. Structures visible on this surface include:
- Right lobe impressions: The right lobe bears impressions of the structures inferiorly adjacent to it — the colic impression (right colic flexure), the renal impression (right kidney and right adrenal), and the duodenal impression (second part of the duodenum, which is retroperitoneal and lies in close apposition to the right lobe).
- Left lobe impressions: The gastric impression — the stomach moulds a concave impression on the under-surface of the left lobe. The oesophageal groove — the abdominal oesophagus marks a small groove at the left margin where it enters the stomach.
- Gallbladder fossa — the gallbladder lies in a shallow fossa on the infero-anterior surface of the right lobe, to the right of the quadrate lobe. The gallbladder receives its blood supply from the cystic artery (most commonly a branch of the right hepatic artery in Calot’s triangle) and drains directly into the liver via small biliary branches through the gallbladder bed.
- Quadrate lobe — bounded on the right by the gallbladder fossa, on the left by the fissure for the ligamentum teres (round ligament), anteriorly by the inferior border, and posteriorly by the porta hepatis. Despite appearing central, this lobe is functionally segment IV of the left liver (see Couinaud section).
- Caudate lobe — bounded on the right by the groove for the IVC, on the left by the fissure for the ligamentum venosum, and anteriorly by the porta hepatis. It is located posteriorly and is the most anatomically independent segment (Segment I).
- Porta hepatis (the crossbar of the H) — the transverse fissure between the quadrate and caudate lobes through which the portal triad enters: the portal vein (posteriorly), the hepatic artery (anteriorly and to the left), and the hepatic bile duct (anteriorly and to the right).
The visceral surface is marked by an H-shaped pattern of fissures that divides the traditional four lobes:
| Structure | Anatomy | Clinical Note |
|---|---|---|
| Ligamentum teres (round ligament) | Left anterior fissure. Fibrous remnant of the fetal umbilical vein — carried oxygenated blood from the placenta to the fetal liver. | Defines the left boundary of the quadrate lobe. Landmark in hepatic surgery and laparoscopy. |
| Ligamentum venosum | Left posterior fissure. Remnant of the fetal ductus venosus — bypassed the liver, shunting oxygenated umbilical blood directly to the IVC. | Separates the caudate lobe from the left lobe. |
| Gallbladder fossa | Right anterior groove — the gallbladder sits here. | Marks the right boundary of the quadrate lobe. Cantlie’s line passes through it. |
| IVC groove | Right posterior groove — the retrohepatic IVC sits here. | Cantlie’s line connects gallbladder fossa to IVC groove — defines functional left/right livers. |
| Porta hepatis | The crossbar of the H — transverse fissure on the visceral surface. Central gateway: portal vein, hepatic artery, and hepatic duct all enter/exit here. | The hepatoduodenal ligament (free edge of lesser omentum) contains these three structures and is the site of Pringle’s manoeuvre. |
| Falciform ligament | Connects the anterior surface of the liver to the anterior abdominal wall. Contains the ligamentum teres in its free inferior edge. | Visible on laparoscopy as the midline peritoneal fold. Used as a landmark to identify the left lobe. |
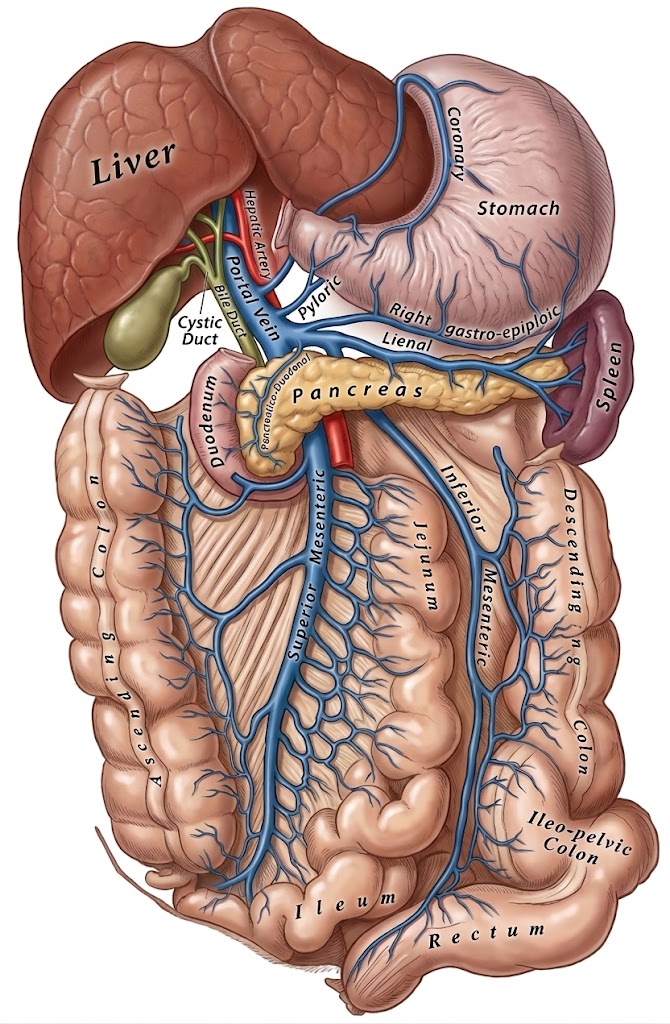
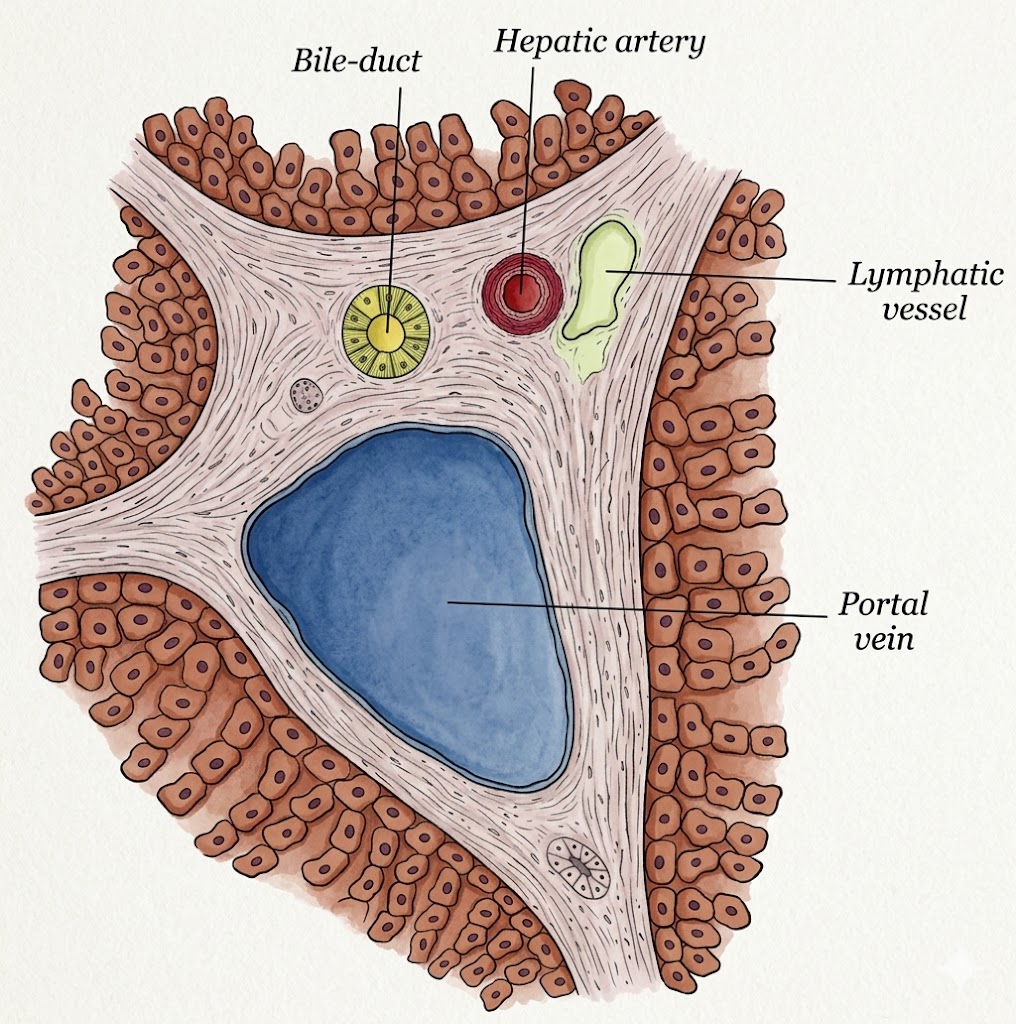
Portal vein formation from the union of the SMV and splenic vein, and the arrangement of structures within the porta hepatis
The portal vein is formed by the union of the superior mesenteric vein (SMV) and the splenic vein behind the neck of the pancreas (at the level of L1–L2). The inferior mesenteric vein typically drains into the splenic vein before this junction. The portal vein then ascends within the hepatoduodenal ligament (the free edge of the lesser omentum) to reach the porta hepatis, where it divides into left and right branches.
- Tributaries of the splenic vein: Short gastric veins, left gastro-epiploic vein, inferior mesenteric vein (carrying blood from the left colon and rectum), and multiple pancreatic branches.
- Tributaries of the SMV: Jejunal and ileal branches, right gastro-epiploic vein, ileocolic vein, right and middle colic veins — draining the entire small bowel and right/transverse colon.
- The portal vein carries: Nutrient-rich but deoxygenated blood from the entire gastrointestinal tract, spleen, and pancreas — representing ~75–80% of total hepatic blood flow by volume.
Arrangement at the Porta Hepatis
Within the hepatoduodenal ligament and at the porta hepatis, the three components of the portal triad maintain a consistent arrangement that must be recalled for surgery and for Pringle’s manoeuvre:
- Portal vein — lies posteriorly, the largest structure
- Hepatic artery proper — lies anteriorly and to the left
- Common bile duct — lies anteriorly and to the right
A useful mnemonic for the contents of the hepatoduodenal ligament (from anterior to posterior): CBD (right) — Artery (left) — Vein (posterior) — “CAV“.
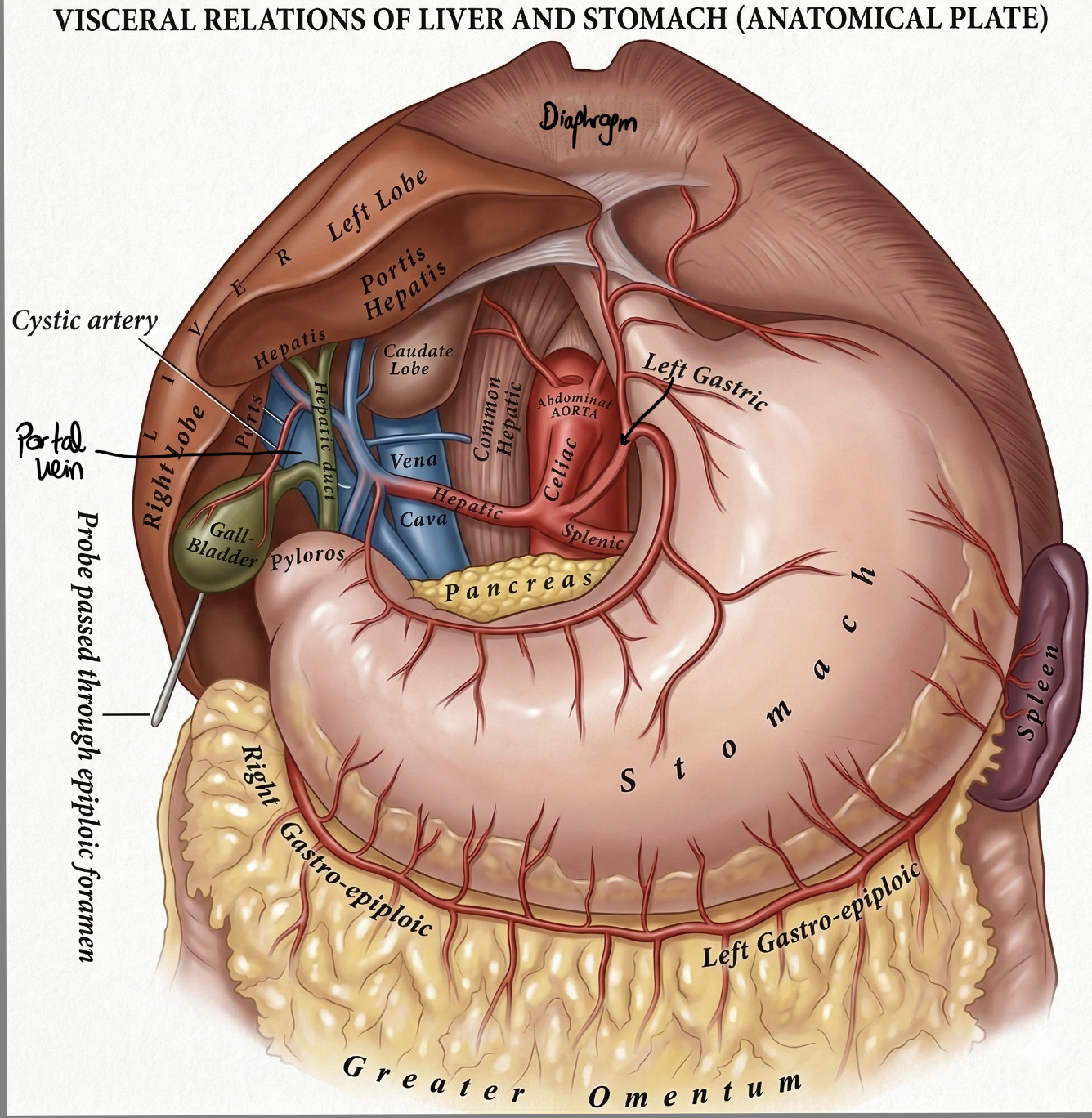
The coeliac trunk and its branches, with the hepatic artery course and porta hepatis labelled
The coeliac trunk (coeliac axis) arises from the abdominal aorta at the level of T12, just below the aortic hiatus of the diaphragm. It is a short, wide vessel (~1–2 cm) that almost immediately divides into its three major branches:
- Left gastric artery — the smallest branch. Ascends to the cardia and supplies the lesser curvature of the stomach and the distal oesophagus. Anastomoses with the right gastric artery along the lesser curvature.
- Splenic artery — the largest branch and the most tortuous artery in the body. Runs along the superior border of the pancreatic body and tail to reach the splenic hilum. Gives off numerous pancreatic branches, the left gastro-epiploic artery, and short gastric arteries.
- Common hepatic artery — runs to the right toward the liver. Gives off the gastroduodenal artery (GDA) before becoming the proper hepatic artery, which then ascends in the hepatoduodenal ligament to the porta hepatis.
Course of the Hepatic Artery
- Common hepatic artery → passes along the superior border of the first part of the duodenum
- Gives off the gastroduodenal artery (GDA) — which passes behind D1 to supply the head of the pancreas (superior pancreaticoduodenal artery) and the first part of the duodenum. The GDA is the vessel under-run in a posterior duodenal ulcer.
- Right gastric artery — small branch to the lesser curvature
- Proper hepatic artery — ascends in the hepatoduodenal ligament (anterior and to the left of the CBD, anterior to the portal vein)
- Divides into right hepatic artery (passes posterior to the common hepatic duct and enters Calot’s triangle to give the cystic artery before entering the liver) and left hepatic artery
Pringle’s Manoeuvre — Controlling Hepatic Inflow
Pringle’s manoeuvre involves manually compressing the hepatoduodenal ligament between the surgeon’s index finger (in the foramen of Winslow, the opening into the lesser sac) and thumb to occlude the portal triad — simultaneously stopping portal vein and hepatic artery inflow to the liver. Used to control haemorrhage during liver surgery or trauma.
Tolerated for up to 15–20 minutes in a normal liver; significantly less in a cirrhotic liver (which is much more sensitive to warm ischaemia). The portal vein (posterior), hepatic artery (anterior-left), and CBD (anterior-right) are all compressed together within the hepatoduodenal ligament.
Intermittent Pringle (15 min clamp / 5 min release cycles) is preferred over continuous clamping to reduce ischaemia-reperfusion injury.
The traditional four-lobe description (based on external anatomy) does not reflect independent vascular supply or bile drainage, and therefore has no surgical relevance. The functional division is what matters:
| System | Division | Boundary |
|---|---|---|
| Traditional (surface anatomy) | Right lobe, Left lobe, Caudate lobe, Quadrate lobe | Based on external fissures — does NOT reflect independent vasculature |
| Cantlie’s line (functional) | Functional right liver (segments V–VIII) and functional left liver (segments I–IV) | Imaginary plane from the gallbladder fossa → IVC. The middle hepatic vein runs along this plane. |
The Surgical Trick — Where is the Quadrate Lobe?
The quadrate lobe (between the gallbladder fossa and the ligamentum teres) appears to belong to the right liver by surface anatomy. However, it receives its portal blood supply from the left portal vein and drains bile into the left hepatic duct — making it functionally segment IV of the left liver. This is a classic MRCS viva question. The practical implication: a right hemihepatectomy along Cantlie’s line preserves the quadrate lobe.
Henri Couinaud (1957) divided the liver into 8 independent functional segments, each with its own portal pedicle (portal vein branch + hepatic artery branch + bile duct branch) and drained by a hepatic vein. Any segment can theoretically be resected independently — the basis of all modern liver surgery.
- I
Caudate Lobe — The Independent Segment
Unique anatomy: receives portal blood from both left and right portal veins; drains bile to both hepatic ducts. Most importantly, its venous outflow consists of short hepatic veins directly into the IVC — bypassing the main hepatic veins entirely. This independent drainage causes compensatory caudate hypertrophy in Budd-Chiari syndrome (hepatic vein thrombosis) — the caudate continues draining normally while the rest of the liver becomes congested. An enlarged caudate on imaging in the right clinical context is pathognomonic.
- II–III
Left Lateral Section
Supplied by the left portal vein, drained by the left hepatic vein. Anatomically the left lobe visible on the surface. Used for left lateral sectionectomy (segments II+III) — the most common living donor hepatectomy for paediatric liver transplantation.
- IV
Quadrate Lobe — Functionally LEFT, Anatomically Between Fissures
Between the gallbladder fossa (right) and ligamentum teres (left). Despite its central anatomical position, it receives its portal supply from the left portal vein → functional segment IV of the left liver. Resected with the left liver in left hemihepatectomy.
- V–VIII
Right Liver — Four Segments
V and VIII are the anterior section (right hepatic artery + portal branch, drained by middle hepatic vein). VI and VII are the posterior section (right portal vein posterior branch, drained by right hepatic vein). The right hepatic vein separates anterior from posterior sections within the right liver.
| Vessel | Contribution | Key Facts |
|---|---|---|
| Portal vein (75–80%) | Nutrient-rich but deoxygenated blood from GI tract, pancreas, spleen | Formed by SMV + splenic vein behind the pancreatic neck. Despite being venous blood, it is highly metabolically important — contains absorbed nutrients, drugs, bacterial products. Lies posteriorly in the hepatoduodenal ligament. |
| Hepatic artery (20–25%) | Well-oxygenated arterial blood via common hepatic artery from the coeliac axis | Despite the smaller volume, the hepatic artery supplies most of the oxygen. Supplies the bile ducts — hepatic artery thrombosis post-transplant causes biliary ischaemia. Lies anterior and medial in the hepatoduodenal ligament (to the left of the CBD). |
| Hepatic veins (outflow) | Three main veins (right, middle, left) drain processed blood back to systemic circulation | Do NOT exit at the porta hepatis. They drain from the posterior surface directly into the retrohepatic IVC just below the diaphragm. The middle hepatic vein runs along Cantlie’s line. Short hepatic veins from the caudate drain directly into the IVC. |
Liver histology showing the hepatic lobule structure — portal triads at the periphery, sinusoids running between hepatocyte plates, and the central hepatic venule
The functional unit of the liver is the hepatic lobule — a hexagonal structure ~1 mm in diameter. Portal triads (containing a portal vein branch, hepatic artery branch, and bile ductule) occupy the six peripheral corners; the central hepatic venule (intralobular vein, draining into a hepatic vein) sits at the centre. Blood flows inward from the portal triads at the periphery toward the central vein. Bile flows in the opposite direction — outward from the centre toward the portal triads.
Key Microscopic Structures
- Hepatocytes — the metabolic workhorses of the liver, arranged in one-cell-thick plates (or cords) radiating from the central vein toward the portal triads. Responsible for synthesis (albumin, clotting factors, glucose, cholesterol), detoxification (ammonia → urea, drug metabolism), and bile production.
- Sinusoids — specialised, fenestrated capillaries running between the hepatocyte plates, from the portal triads inward to the central vein. Their fenestrated endothelium (unlike regular capillaries) allows direct contact between plasma and hepatocytes — maximising metabolic exchange. Blood entering the sinusoids is a mixture of portal venous blood (nutrient-rich) and hepatic arterial blood (oxygen-rich).
- Kupffer cells — the liver’s resident macrophages, lining the sinusoidal endothelium. They phagocytose bacteria, damaged RBCs, cellular debris, and particulate matter arriving from the portal circulation. Kupffer cells are activated in sepsis, alcoholic hepatitis, and NAFLD, releasing pro-inflammatory cytokines that contribute to hepatocyte injury and fibrosis.
- Space of Disse — the narrow perisinusoidal space between the fenestrated sinusoidal endothelium and the hepatocyte surface. Plasma percolates freely into this space, giving hepatocytes direct access to plasma proteins and substrates. Hepatic stellate cells (Ito cells) reside here in their quiescent state, storing vitamin A (retinol) as lipid droplets. When activated by chronic liver injury (alcohol, viral hepatitis, NAFLD), stellate cells transform into myofibroblasts → deposit type I collagen → progressive hepatic fibrosis → cirrhosis. The Space of Disse collapses in cirrhosis (capillarisation of sinusoids), reducing the fenestrations and impairing hepatocyte function.
- Bile canaliculi — tiny tubular channels formed by the apical membranes of adjacent hepatocytes (not a separate structure — created by the groove between two hepatocytes). Bile secreted by hepatocytes flows along these canaliculi in the opposite direction to blood (outward, from the central vein region toward the portal triads), collecting into the bile ductules (canals of Hering) at the portal triad, then into the interlobular bile ducts, and ultimately the left and right hepatic ducts.
- Glisson’s capsule — the dense fibrous connective tissue capsule that surrounds the entire liver. Continuous with the peritoneal covering. The perivascular fibrous sheaths (also called Glisson’s sheath) extend from this capsule into the liver parenchyma around the portal triads, carrying the portal vein, hepatic artery, and bile duct branches together as they ramify through the liver. Its distension from acute hepatic enlargement (hepatitis, right heart failure, Budd-Chiari) causes the characteristic dull, constant right upper quadrant aching pain.
Zones of the Hepatic Acinus — Why Certain Injuries Are Zone-Specific
Rappaport described the liver in terms of acinar zones based on oxygen and nutrient delivery from the portal triad (Zone 1) to the central vein (Zone 3):
🔵 Zone 1 (periportal) — closest to the portal triad. Receives blood with the highest oxygen and nutrient content. First exposed to toxins arriving from the portal circulation. Zone 1 injury occurs in: phosphorus poisoning, eclampsia, yellow fever.
🔵 Zone 2 (midzonal) — intermediate zone. Injured in: yellow fever (characteristic midzonal necrosis).
🔵 Zone 3 (centrilobular / perivenular) — furthest from the portal triad. Receives the most deoxygenated blood and is most susceptible to ischaemic injury and toxic damage. Zone 3 injury occurs in: paracetamol (acetaminophen) overdose (CYP2E1 — the enzyme that converts paracetamol to the toxic NAPQI metabolite — is concentrated in Zone 3), alcoholic hepatitis (centrilobular necrosis + Mallory bodies), and ischaemic hepatitis (right heart failure, shock → centrilobular congestion and necrosis — “nutmeg liver”).
Practical pearl: In paracetamol overdose, ALT peaks at 72–96 hours as Zone 3 necrosis progresses. The characteristic histological finding is centrilobular (Zone 3) haemorrhagic necrosis with relative sparing of Zone 1.