🔴 Oesophagus
Anatomy & physiology, GORD, hiatus hernias, achalasia & motility disorders, pharyngeal pouch, Barrett’s oesophagus, oesophageal carcinoma, Boerhaave’s syndrome, and oesophagectomy approaches.
Oesophageal Anatomy & Physiology
The oesophagus is a 25 cm muscular tube running from the cricopharyngeal sphincter at C6 to the gastro-oesophageal junction (GOJ) at T10. On endoscopy, the GOJ lies approximately 40 cm from the incisors.
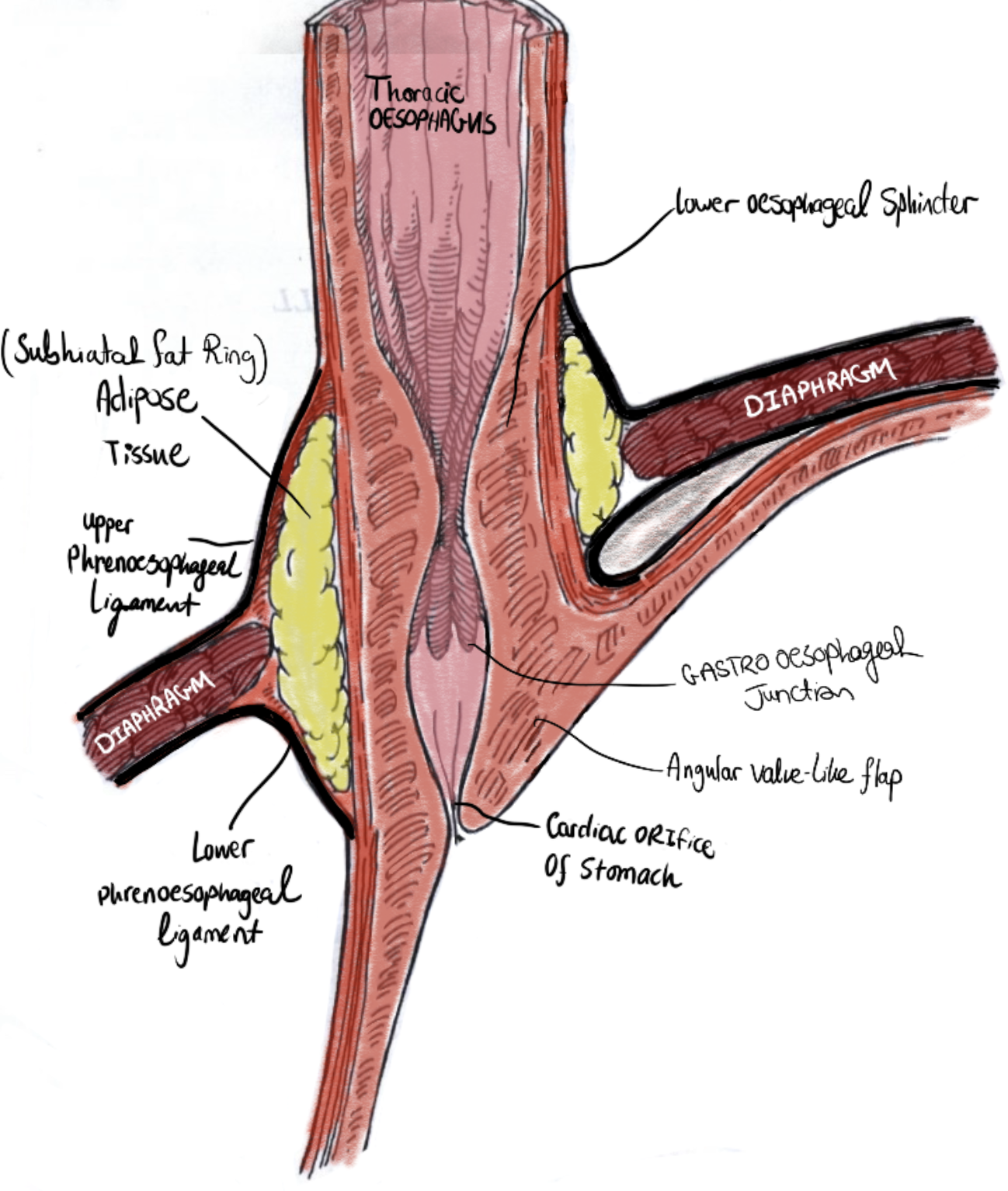
Gastro-oesophageal junction (GOJ) and lower oesophagus — anatomical relations, Z-line, right crus of diaphragm, and angle of His
The “No Serosa” Rule — The Most Important Surgical Fact
Unlike every other part of the GI tract, the oesophagus lacks a serosal layer. This has profound surgical consequences:
🔴 Sutures hold poorly — anastomoses are technically demanding and prone to failure
🔴 Anastomotic leak risk is high — an Ivor Lewis leak dumps contents directly into the mediastinum; potentially lethal
🔴 Tumour spreads early — without the serosal barrier, oesophageal cancer invades adjacent structures (aorta, trachea, spine) early
🔴 No fibrin seal after perforation — Boerhaave’s rapidly causes mediastinitis with no serosal containment
| Layer | Structure | Clinical Significance |
|---|---|---|
| Mucosa | Stratified squamous epithelium (changes to columnar at the Z-line/GOJ) | Barrett’s oesophagus = columnar metaplasia replacing squamous epithelium; adenocarcinoma risk |
| Submucosa | Dense connective tissue with vessels, lymphatics, Meissner’s plexus | Rich longitudinal lymphatics explain skip metastases in oesophageal cancer |
| Muscularis propria | Inner circular + outer longitudinal. Upper 1/3 = striated; middle = mixed; lower = smooth. Auerbach’s (myenteric) plexus between the two layers. | Auerbach’s plexus destruction → achalasia. Upper striated muscle affected by myasthenia, MND. |
| Adventitia | Loose connective tissue — NO serosa | Absent serosa = rapid tumour spread, high anastomotic leak morbidity |
Measured from the incisors. Sites where foreign bodies lodge, strictures form, tumours preferentially arise, and perforations occur during endoscopy.
-
15 cm
Cricopharyngeal Sphincter (UOS / C6)
Entry to the oesophagus. Most common site of iatrogenic perforation during rigid endoscopy. Zenker’s pharyngeal pouch forms just above here (Killian’s dehiscence). Post-cricoid web (Plummer-Vinson) forms here.
-
22 cm
Aortic Arch Crossing (T4)
Left lateral indentation. Foreign bodies lodge here. Aortic aneurysms cause extrinsic compression. Upper/middle third tumours invading laterally may involve the aorta — unresectable.
-
27 cm
Left Main Bronchus / Carina (T5)
External indentation. Carinal and subcarinal nodes frequently involved in cancer. Tumours here may invade the trachea/bronchus → oesophago-respiratory fistula — Ono’s sign (coughing on swallowing) = unresectable.
-
40 cm
Diaphragmatic Hiatus / GOJ (T10)
Most clinically important narrowing. GOJ marked by the squamocolumnar Z-line — site of Barrett’s metaplasia, adenocarcinoma, reflux, and hiatus hernia. The right crus pinchcock contributes to LOS competence.
| Level | Aperture | Contents | Memory Aid |
|---|---|---|---|
| T8 | Caval hiatus | IVC + right phrenic nerve | “8 letters in vena cava” |
| T10 | Oesophageal hiatus | Oesophagus + left & right vagal trunks + left gastric vessels | “10 letters in oesophagus” |
| T12 | Aortic hiatus | Aorta + thoracic duct + azygous vein | “12 letters in aortic hiatus” |
| Region | Arterial Supply | Venous Drainage | Key Clinical Point |
|---|---|---|---|
| Upper 1/3 | Inferior thyroid artery (thyrocervical trunk) | Inferior thyroid vein → brachiocephalic vein | Segmental — extensive mobilisation risks devascularisation → anastomotic ischaemia. Cervical oesophagus most vulnerable in McKeown. |
| Middle 1/3 | Direct aortic branches + right bronchial artery | Azygous vein | Azygous vein divided during right thoracotomy (Ivor Lewis). Must identify carefully to avoid haemorrhage. |
| Lower 1/3 | Left gastric artery (coeliac axis) | Left gastric vein → portal vein | Portosystemic anastomosis. Portal hypertension → retrograde flow → oesophageal varices. |
Mnemonic: “I Dare Leave” — Blood Supply Upper to Lower
Inferior thyroid artery — Upper third (from thyrocervical trunk)
Direct aortic branches — Middle third
Left gastric artery — Lower third (from coeliac axis)
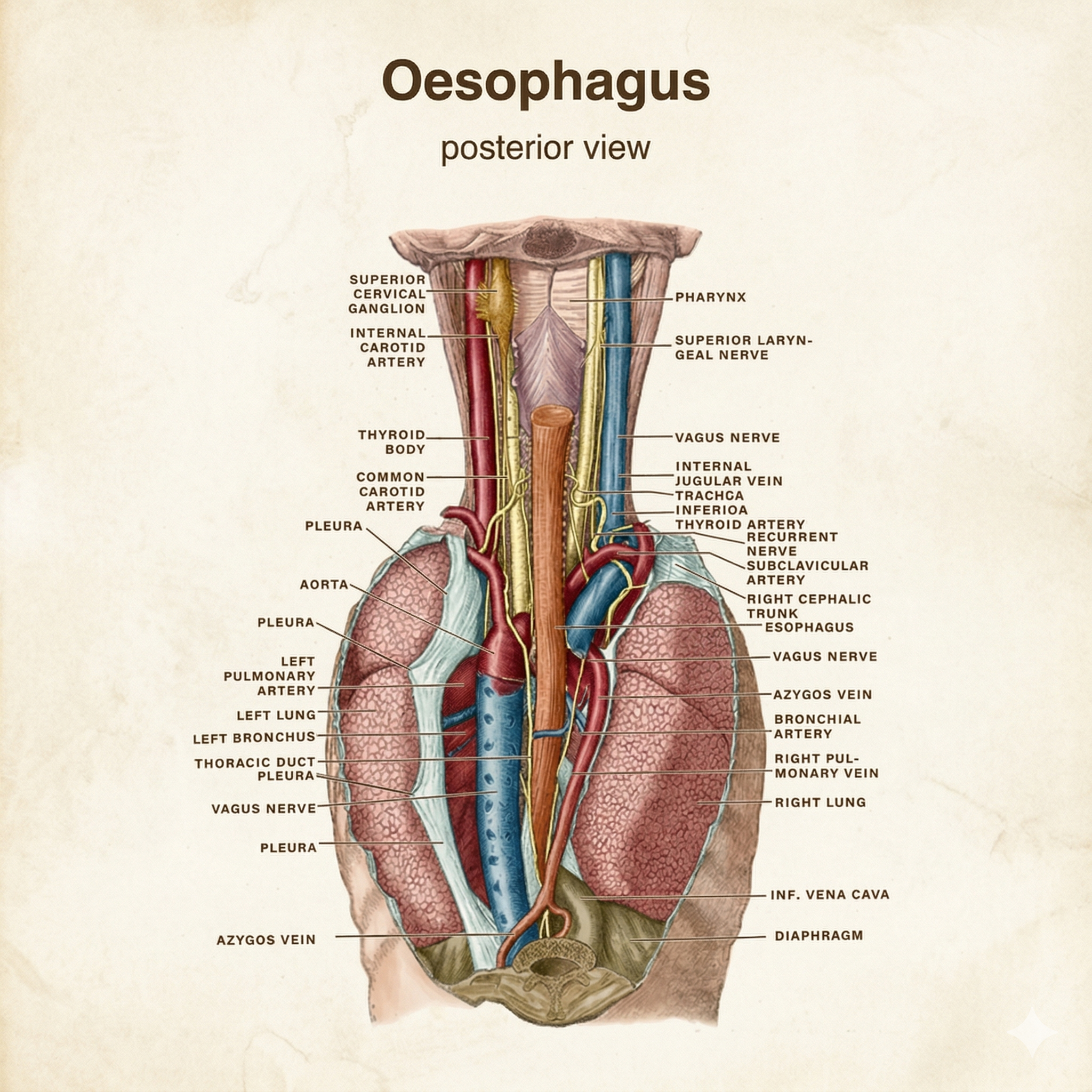
Thoracic aorta (posterior view) — showing the direct aortic oesophageal branches supplying the middle third, the azygous vein, and the thoracic duct. The left main bronchus and aortic arch are key landmarks for the constrictions at 22 cm and 27 cm.
The LOS is a physiological rather than anatomical sphincter — no discrete ring of muscle at the GOJ. Resting LOS pressure is 10–15 mmHg. Competence is maintained by four mechanisms:
- Intrinsic smooth muscle tone — reduced by progesterone, fatty meals, alcohol, caffeine, nitrates, calcium channel blockers.
- Pinchcock action of the right crus of the diaphragm — tightens during inspiration. Disrupted by hiatus hernia.
- Angle of His — acute angle between oesophagus and gastric greater curve creates a flap valve. Widened by GOJ herniation.
- Intra-abdominal segment of oesophagus — positive intra-abdominal pressure compresses it shut. Lost when GOJ herniates above the diaphragm.
- 1Oral phase (voluntary): Bolus formed; tongue propels bolus into oropharynx.
- 2Pharyngeal phase (involuntary — CN IX/X): Soft palate elevation seals nasopharynx; laryngeal elevation + epiglottic retroflexion + vocal cord adduction protect airway; UOS (cricopharyngeus) relaxes. Coordinated by brainstem swallowing centre in the medulla.
- 3Oesophageal phase (involuntary, peristaltic): Primary peristalsis propels bolus. Secondary peristalsis triggered by oesophageal distension (clears refluxate). Tertiary contractions = non-propulsive and pathological.
The Vagus Nerve — The Surgical Trap
The vagus nerves undergo a 90° rotation as the stomach rotates embryologically:
🔵 Left vagus → runs anteriorly on the lower oesophagus and GOJ
🔵 Right vagus → runs posteriorly
Bilateral injury causes gastroparesis, post-vagotomy diarrhoea, and dumping — recognised late and difficult to treat. Always identify and protect both vagal trunks at the GOJ.
| Region | Primary Lymph Node Drainage | Clinical Implication |
|---|---|---|
| Upper third | Deep cervical nodes | Cervical lymphadenopathy from upper oesophageal tumours |
| Middle third | Mediastinal / tracheobronchial nodes | Mediastinal spread — hoarseness (RLN), tracheal involvement |
| Lower third | Coeliac nodes | Abdominal node involvement from lower oesophageal / GOJ cancers |
Skip Metastasis — Why PET-CT is Mandatory
Oesophageal lymphatics run longitudinally within the submucosa before draining regionally — tumour cells travel considerable distances before reaching a regional lymph node. A mid-oesophageal tumour may have cervical or coeliac lymph node metastases with no involved mediastinal nodes. PET-CT is mandatory in staging — CT alone misses ~20% of patients with occult distant nodal disease.