🟢 The Small Bowel
Anatomy · Physiology & Absorption · Bowel Viability · Obstruction · Meckel’s Diverticulum · Crohn’s Disease · Short Bowel & Ileostomy · Ischaemia & Fistulas · Tumours — MRCS Part A & B
Small Bowel Anatomy
The small intestine is the principal site for digestion and absorption, extending approximately 6–7 metres from the pylorus to the ileocaecal valve. It is divided into three segments: the duodenum, jejunum, and ileum.
The duodenum is the first, widest, and shortest segment (~25 cm — “twelve finger breadths”). C-shaped, curling around the head of the pancreas. Almost entirely retroperitoneal except for the first 2 cm (duodenal cap/bulb), which has a mesentery and is mobile.
- D1
Superior / First Part (Duodenal Cap / Bulb)
Begins at the pylorus, runs posterosuperiorly. The first 2 cm is mobile. Most common site for peptic ulceration. The gastroduodenal artery (GDA) lies immediately posterior — a posteriorly perforating D1 ulcer bleeds from the GDA.
- D2
Descending / Second Part
Descends on the right side of the spine. Contains the major duodenal papilla (Ampulla of Vater) on its posteromedial wall — the opening of the common bile duct and main pancreatic duct (Wirsung). Also contains the minor papilla (accessory duct of Santorini). Pancreatic head carcinoma compresses the CBD here → obstructive jaundice.
- D3
Horizontal / Third Part
Crosses the midline horizontally. Passes between the aorta posteriorly and the SMA anteriorly — basis of SMA syndrome. With extreme weight loss, the fat pad between SMA and aorta disappears, narrowing the aortomesenteric angle → compression of D3 → proximal obstruction.
- D4
Ascending / Fourth Part
Ascends to the left to reach the duodenojejunal (DJ) flexure, supported by the ligament of Treitz (fibromuscular band connecting DJ flexure to the right crus of the diaphragm). The DJ flexure marks the start of the midgut. Upper GI bleeds are proximal to the DJ flexure; lower GI bleeds are distal.
The Ligament of Treitz — The Key Landmark
Fixes the DJ flexure to the right crus of the diaphragm, tethering the duodenum. Critical landmark for:
🔵 Upper vs Lower GI bleed: proximal = upper (haematemesis ± malaena); distal = lower (PR blood)
🔵 Nasojejunal tube placement: tip must be beyond the DJ flexure for post-pyloric feeding
🔵 Ladd’s procedure (malrotation): the ligament of Treitz is released to straighten and fix the duodenum; Ladd’s bands obstructing the duodenum are divided

The Jejunum — Key Distinguishing Features
Thick, heavy wall · Deep red/rose colour (more vascular) · Large, closely packed plicae circulares (“stacked coins”) · Long vasa recta · Few, large arterial arcades (1–2 tiers) · Less mesenteric fat (vessels visible through mesentery) · No Peyer’s patches · Left and upper abdomen
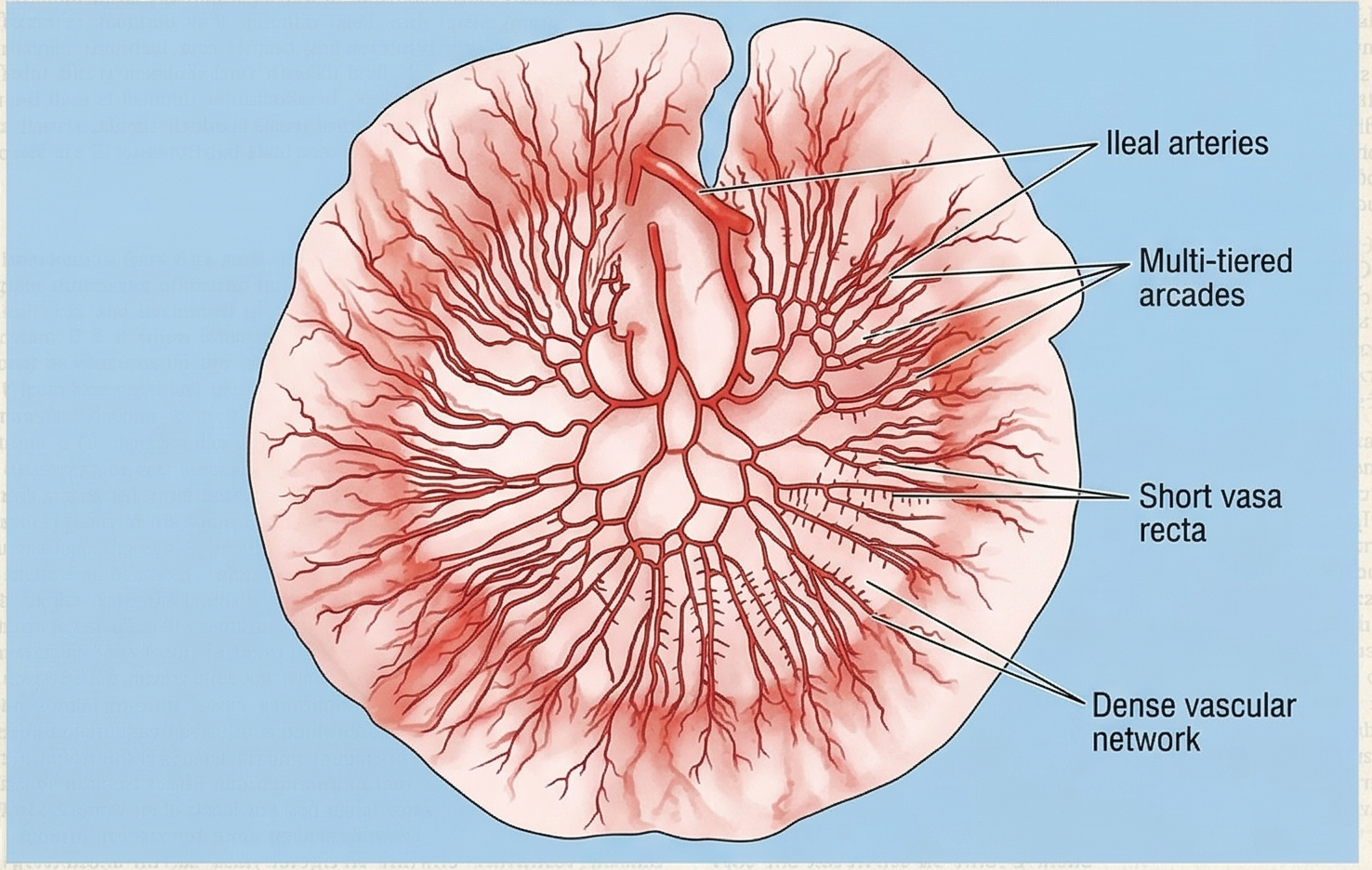
The Ileum — Key Distinguishing Features
Thin, soft wall · Paler pink (less vascular) · Low/absent plicae circulares distally · Short vasa recta · Many, short arterial arcades (3–5 tiers) · More mesenteric fat (“creeping fat” in Crohn’s) · Peyer’s patches present (raised oval lymphoid plaques) · Right and lower abdomen, ends at ileocaecal valve
The jejunum (~2/5 of post-duodenal small bowel) and ileum (~3/5) are suspended from the posterior abdominal wall by the fan-shaped mesentery, which contains the SMA, SMV, lymphatics, and autonomic nerves. There is no fixed external landmark distinguishing them — identification relies on the features below.
| Segment | Arterial Supply | Venous Drainage | Notes |
|---|---|---|---|
| Proximal duodenum (D1–D2 above ampulla) | Gastroduodenal artery → superior pancreaticoduodenal artery (coeliac trunk territory) | Portal vein | Foregut–midgut watershed at the ampulla of Vater. Dual arterial supply protects against ischaemia. |
| Distal duodenum (D2 below ampulla, D3, D4) | SMA → inferior pancreaticoduodenal artery | SMV → portal vein | Midgut territory. Pancreaticoduodenal arcade connects coeliac + SMA — important collateral in aortic surgery. |
| Jejunum & ileum | SMA → 15–18 jejunal/ileal branches → arterial arcades → vasa recta (end-arteries) | SMV → portal vein | Vasa recta are end-arteries with no collateral — injury causes a localised ischaemic segment. |
| Terminal ileum | Ileocolic artery (terminal branch of SMA) | Ileocolic vein → SMV | Most consistent SMA branch — used as the vascular pedicle in right hemicolectomy. |
- Sympathetic (T8–T10): Inhibit peristalsis and secretion; vasoconstriction. Afferent pain fibres travel with the sympathetics → periumbilical referred pain for midgut pathology (appendicitis, SMA ischaemia).
- Parasympathetic (vagus, CN X): Stimulates peristalsis and secretion. Does NOT carry pain afferents.
- Enteric nervous system: Myenteric plexus (Auerbach’s) — controls motility. Submucosal plexus (Meissner’s) — controls secretion. Functions independently but is modulated by the ANS.