🟡 The Stomach
Complete MRCS revision — anatomy, blood supply, peritoneal attachments, gastric physiology, H. pylori, peptic ulcer disease, gastric outlet obstruction, stress ulcers, gastric carcinoma, bariatric surgery, post-gastrectomy syndromes, and gastric volvulus.
Gastric Anatomy
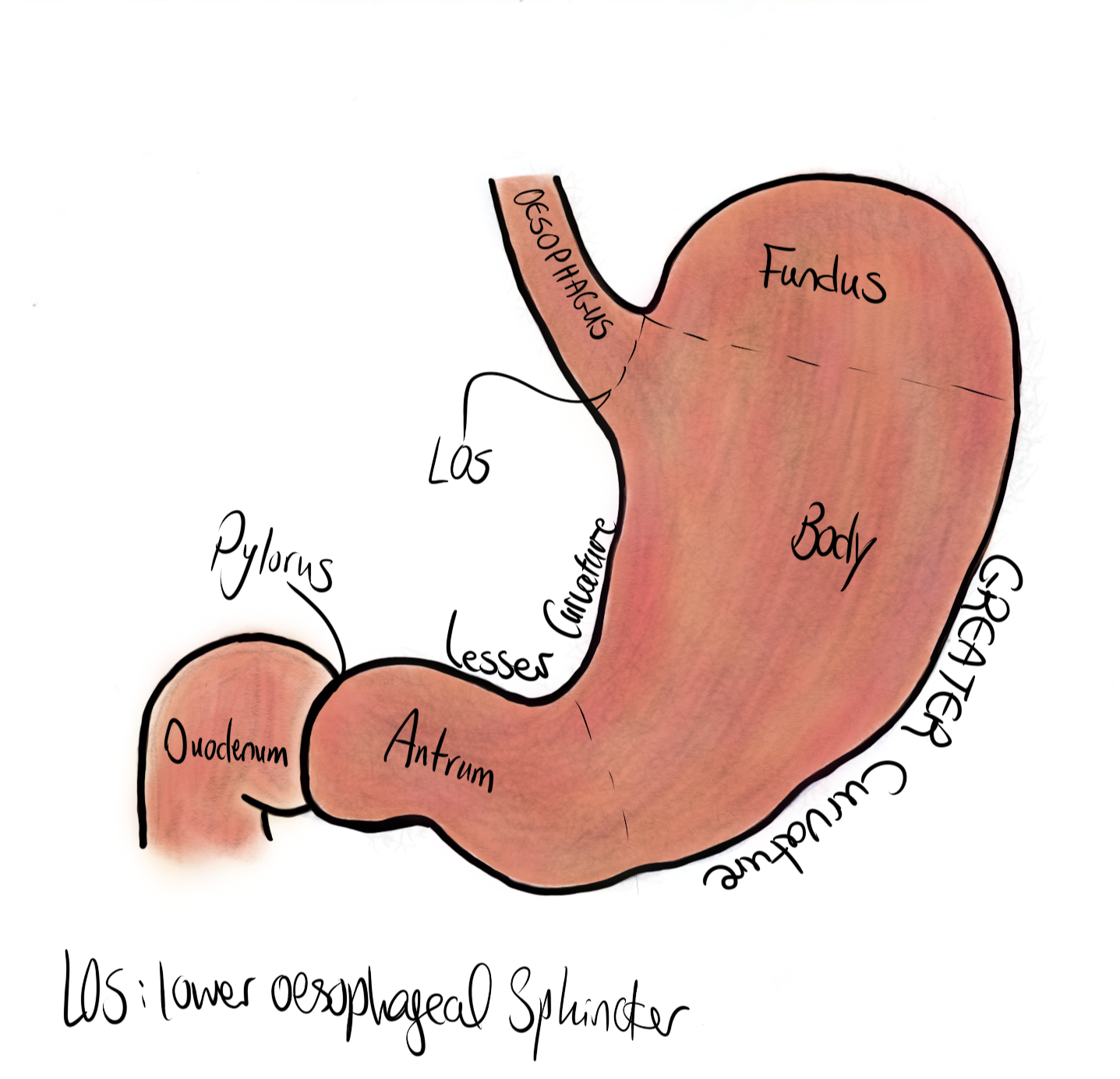
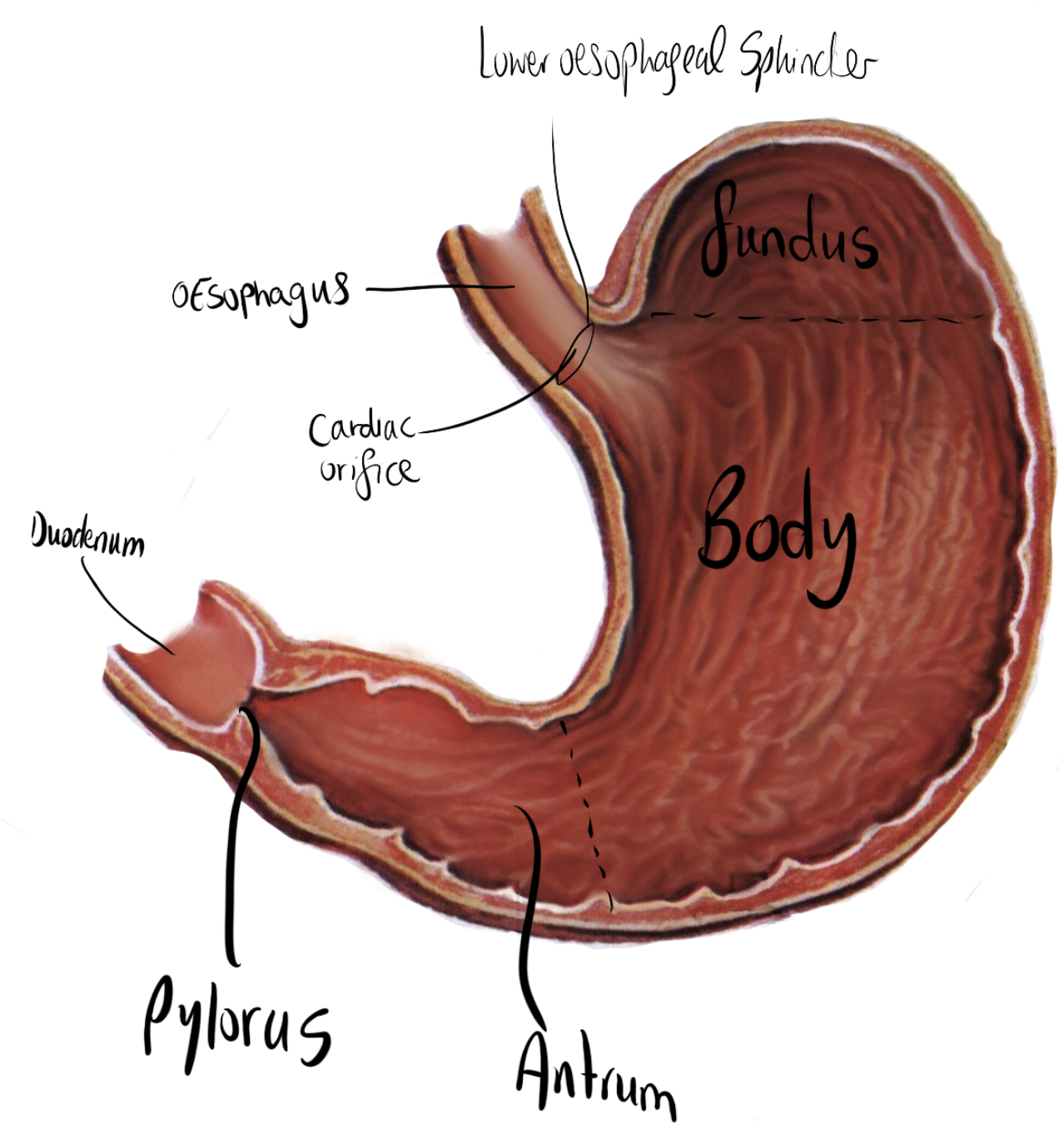
The stomach is divided into five regions from proximal to distal: cardia (GOJ entry zone), fundus (dome above GOJ, contains gas on erect CXR), body (largest part, main secretory zone), antrum (hormonal regulation, pyloric glands), and pylorus (muscular sphincter controlling gastric emptying). The lesser curvature forms the medial border; the greater curvature forms the lateral border.
Lesser Curvature
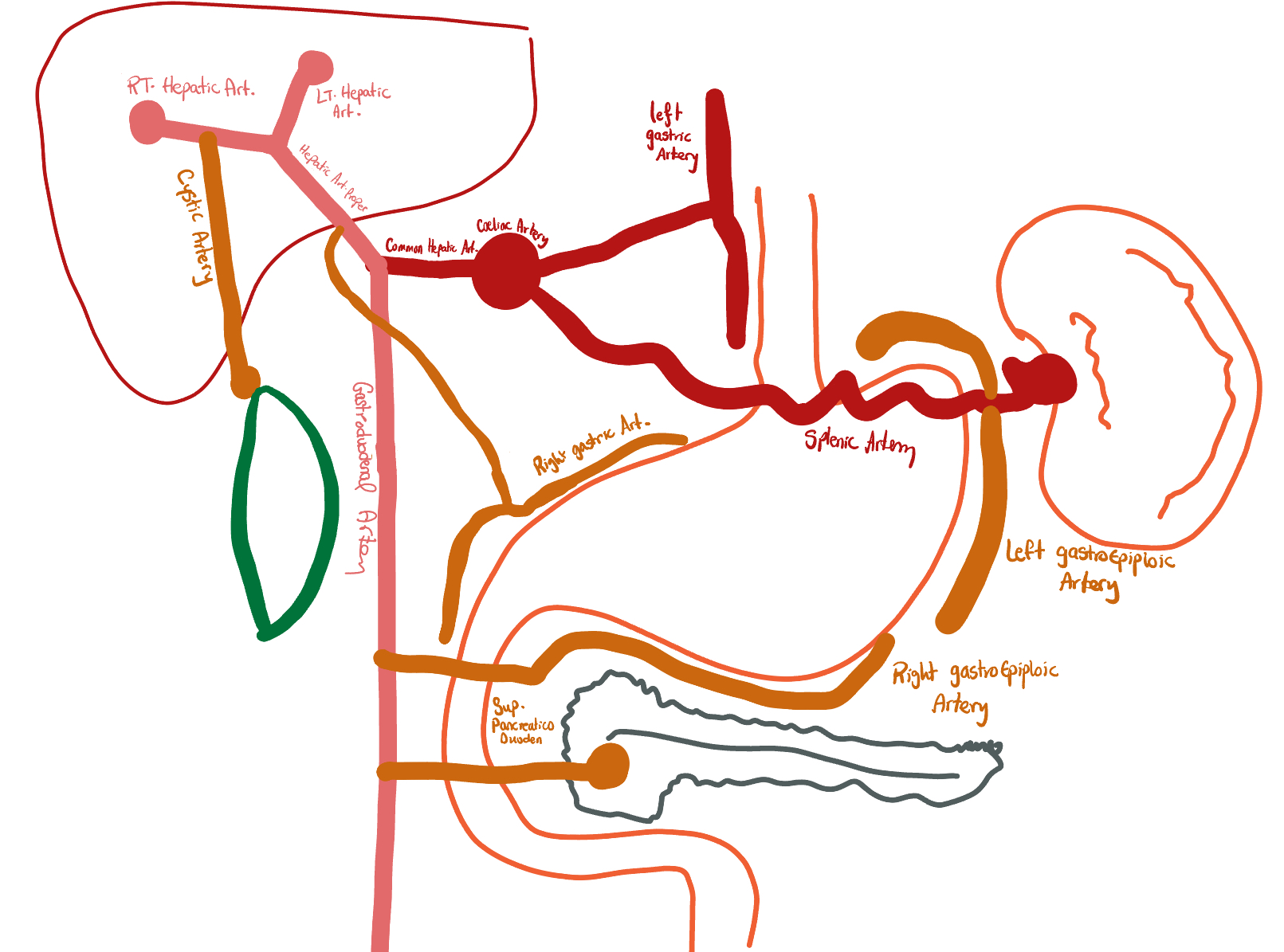
Left + Right gastric arteries
- Left gastric artery — direct branch of the coeliac trunk; largest contributor to lesser curvature; must be ligated during gastrectomy
- Right gastric artery — from the hepatic artery (proper or common)
- These two vessels anastomose along the lesser curvature
Greater Curvature
Left + Right gastroepiploic arteries
- Left gastroepiploic artery — from the splenic artery
- Right gastroepiploic artery — from the gastroduodenal artery (GDA)
- These anastomose along the greater curvature
- The GDA is a branch of the common hepatic artery
Short Gastric Arteries
Gastric fundus
- 4–5 branches from the splenic artery
- Supply the gastric fundus via the gastrosplenic ligament
- Divided during total gastrectomy and splenectomy
- Important: their division = the primary step in mobilising the greater curvature
Venous Drainage
All → portal system
- Left gastric (coronary) vein → portal vein directly
- Right gastric vein → portal vein
- Right gastroepiploic vein → SMV
- Left gastroepiploic + short gastric veins → splenic vein
- Portal hypertension → gastro-oesophageal varices via left gastric vein
Lymphatic Drainage
Follows arterial supply
- Left gastric territory → left gastric nodes → coeliac nodes
- Right gastric territory → hepatic nodes
- Fundus / short gastric territory → splenic nodes
- Lesser curve overall → left gastric → coeliac
- D2 dissection targets all named nodal stations
Nerve Supply
Vagus + sympathetic
- Parasympathetic — vagus nerve (CN X): secretomotor and motor; left vagus → anterior surface; right vagus → posterior surface
- Sympathetic — coeliac plexus (T6–T9): vasomotor, pain fibres; inhibits motility and secretion
- Intrinsic — Auerbach’s plexus (myenteric) and Meissner’s plexus (submucosal)
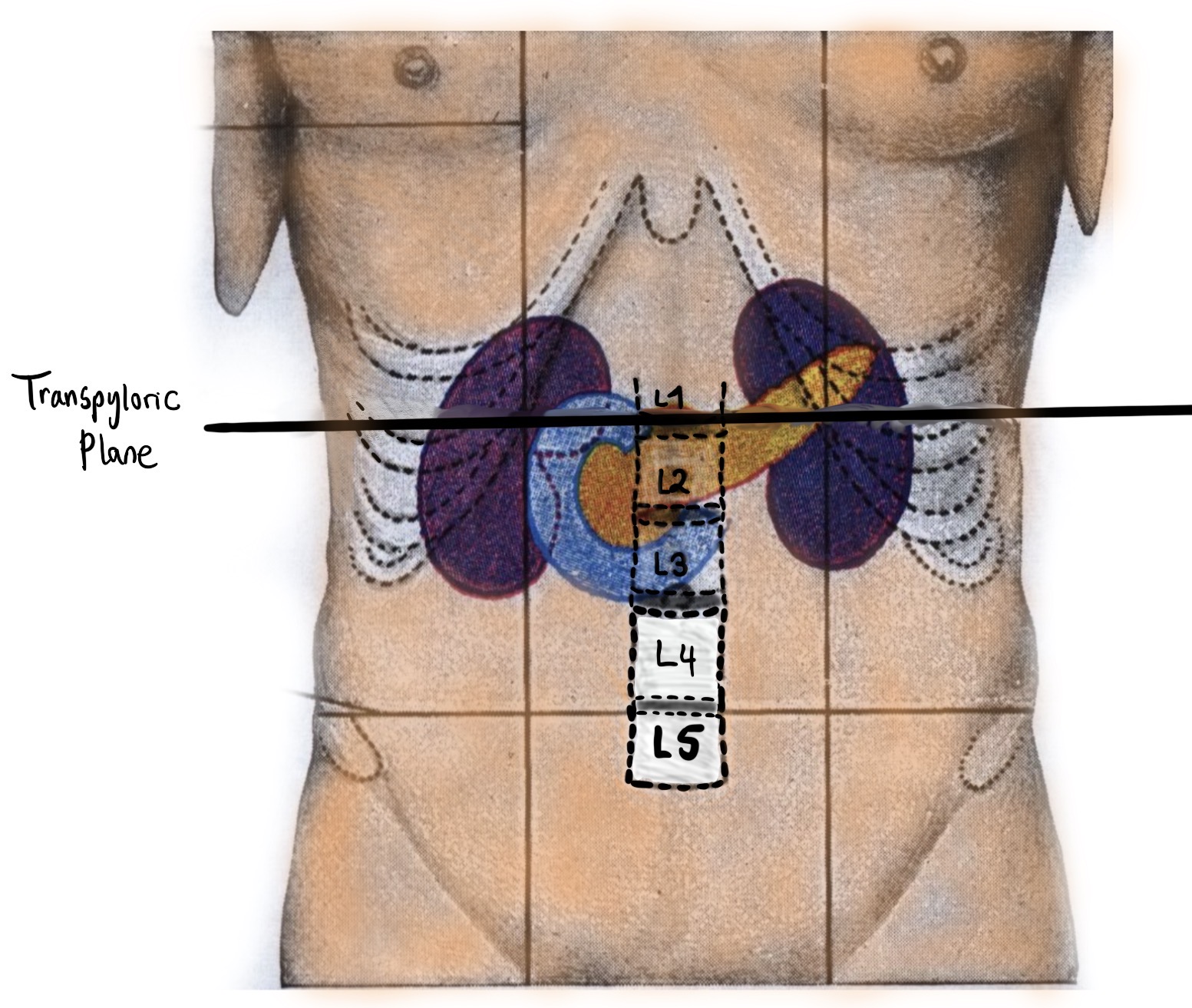
Posterior Relations (Stomach Bed)
Lesser sac lies between stomach and these structures
Mnemonic: PAN SAD — Pancreas · Aorta/splenic artery · (left) Nephric structures · Spleen · Adrenal · Diaphragm (left crus)
- Pancreas — body and tail; posterior gastric ulcer can erode the splenic artery running along the superior pancreatic border
- Splenic artery — tortuous along superior pancreatic border
- Left kidney and adrenal gland
- Transverse mesocolon
- Spleen
Anterior Relations
Covered by peritoneum anteriorly
- Left lobe of liver — overlies the body and lesser curvature
- Anterior abdominal wall — fundus and body directly related when liver is retracted
- Diaphragm — fundus is closely related to the left hemidiaphragm
When an anterior duodenal or gastric ulcer perforates, contents spill into the peritoneal cavity → peritonitis. Free gas collects under the diaphragm on erect CXR.
Lesser Omentum
Hepatogastric + Hepatoduodenal ligaments
Greater Omentum
Gastrocolic, Gastrosplenic, Gastrophrenic
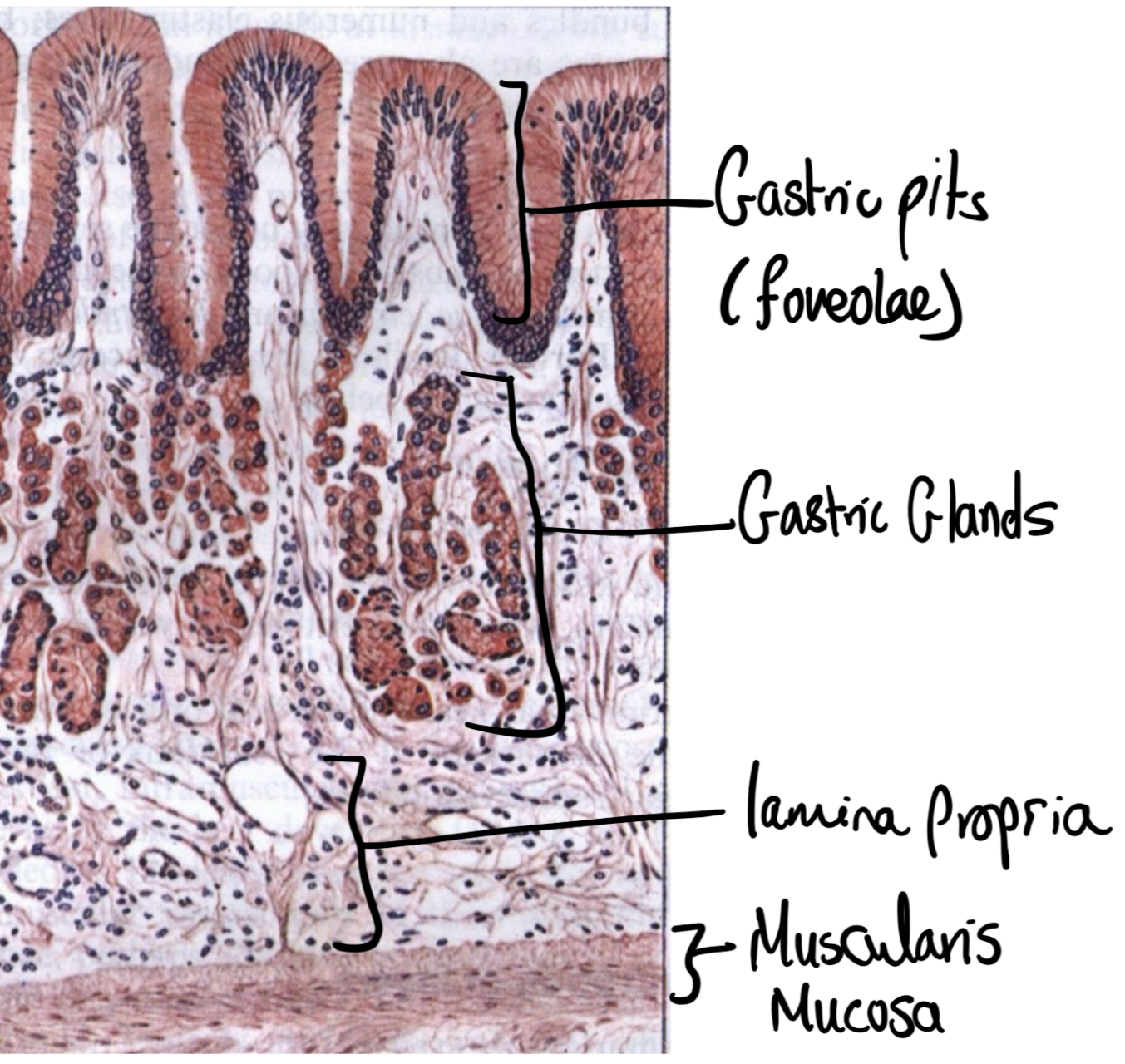
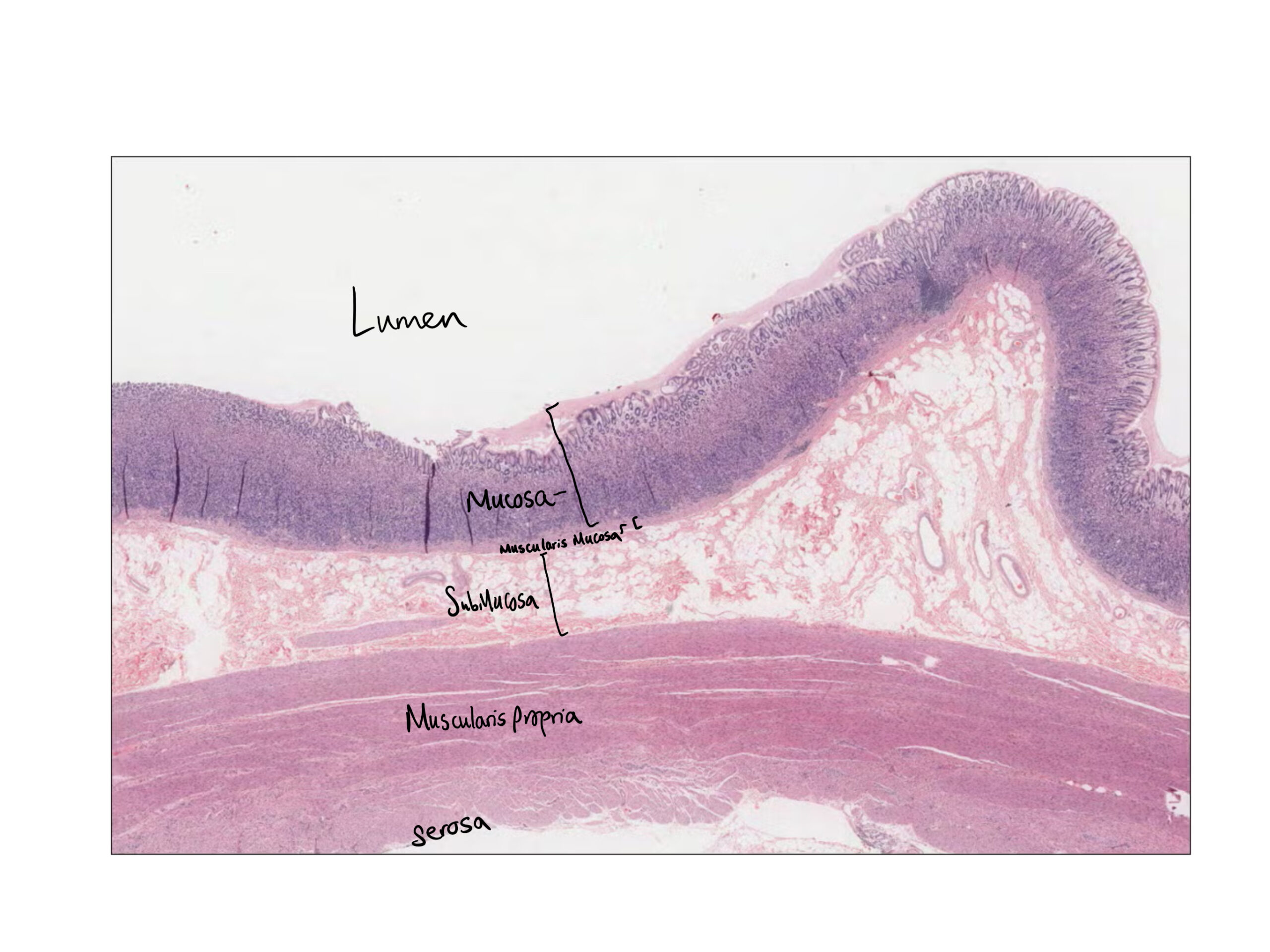
The gastric wall has four layers: mucosa (surface epithelium + gastric glands + lamina propria + muscularis mucosae), submucosa, muscularis externa (oblique inner, circular middle, longitudinal outer — three layers unique to the stomach), and serosa. The mucosa varies by region: body/fundus has deep principal glands packed with parietal and chief cells; the antrum has shallower pyloric glands with G and D cells.
The Lesser Sac (Omental Bursa) — Anatomy and Clinical Relevance
The lesser sac is a potential space posterior to the stomach, bounded anteriorly by the stomach and lesser omentum, posteriorly by the pancreas and stomach bed structures. It communicates with the greater sac via the Epiploic Foramen of Winslow.
Boundaries of the Epiploic Foramen (Winslow):
• Anterior — hepatoduodenal ligament (contains portal triad)
• Posterior — IVC (inferior vena cava)
• Superior — caudate lobe of liver
• Inferior — first part of duodenum
Clinical relevance of the lesser sac:
🔵 Pancreatic pseudocyst — fluid from acute pancreatitis tracks into the lesser sac (it is bounded and cannot easily escape), creating a pseudocyst. Drained into the posterior wall of the stomach (cystgastrostomy) or Roux-en-Y cystjejunostomy.
🔵 Surgical access — the lesser sac is entered via the gastrocolic ligament or lesser omentum to reach the pancreas, the posterior stomach, and the coeliac axis.
🔵 Epiploic foramen herniation — rare but life-threatening internal hernia through the foramen of Winslow.
Gastric volvulus is an abnormal rotation of the stomach around one of its two axes. It may be primary (no anatomical cause — laxity of gastric ligaments) or secondary (paraoeosphageal hernia, diaphragmatic defect, raised left hemidiaphragm). It can be acute (surgical emergency) or chronic (intermittent).
Borchardt’s Triad — Classic Presentation of Acute Gastric Volvulus
1️⃣ Sudden severe epigastric pain — often catastrophic in onset
2️⃣ Violent retching without vomiting — obstruction prevents vomiting
3️⃣ Inability to pass a nasogastric tube — twisted anatomy prevents NG passage
Acute gastric volvulus is a surgical emergency. Ischaemia and strangulation develop rapidly. Management: urgent endoscopic decompression (first-line if viable) or emergency laparotomy with derotation and gastropexy (definitive). Concurrent repair of any diaphragmatic defect or paraosophageal hernia is performed to prevent recurrence.
Organoaxial Volvulus
Most common — rotation around long axis
Mesenteroaxial Volvulus
Less common — rotation around short axis