🦋 Thyroid Gland
Anatomy, embryology, physiology, clinical conditions, thyroid cancers, surgical management and complications — MRCS high-yield.
Anatomy & Embryology
Embryology
The thyroid gland develops from endodermal cells at the base of the tongue — specifically from the foramen caecum (the point where the anterior two-thirds and posterior one-third of the tongue meet). It descends in the midline during weeks 4–7 of gestation via the thyroglossal duct to its final pretracheal position in the neck.
| Embryological Structure | Fate / Clinical Significance |
|---|---|
| Foramen caecum | Origin of thyroid gland — remnant visible as a pit at the junction of anterior 2/3 and posterior 1/3 of tongue dorsum |
| Thyroglossal duct | Normally obliterates after thyroid descent; persistent remnants → thyroglossal cysts or sinuses |
| Thyroglossal cyst | Most common congenital neck swelling in children; midline; moves upward on tongue protrusion (attached to tongue base via tract) and on swallowing; treated by Sistrunk operation (cyst + central hyoid bone excision) |
| Lingual thyroid | Failure of complete descent — thyroid tissue remains at tongue base; may be the patient’s only functioning thyroid; must perform scintigraphy before removing to confirm orthotopic thyroid exists; removal can cause hypothyroidism |
| Parafollicular C-cells | Derived from neural crest cells via ultimobranchial bodies (4th pharyngeal pouch); secrete calcitonin; origin of medullary thyroid carcinoma |
Gross Anatomy
| Feature | Detail |
|---|---|
| Shape | Butterfly-shaped (H-shaped); two lobes connected by the isthmus. A pyramidal lobe extends superiorly from the isthmus in ~50% of people (remnant of thyroglossal duct). |
| Location | Anterior neck at C5–T1; isthmus overlies 2nd–4th tracheal rings. The isthmus is palpated and auscultated for bruits in thyrotoxicosis. |
| Weight | ~25–30 g in adults; each lobe ~4 × 2 × 2 cm |
| Capsule | Enclosed in pretracheal fascia (true capsule). The thyroid moves on swallowing — allows clinical distinction of thyroid from non-thyroid neck masses. |
| Berry’s ligament | Posterior suspensory ligament fixing the thyroid to the cricoid cartilage and tracheal rings — the RLN passes immediately adjacent as it enters the larynx; most vulnerable point during thyroidectomy |
| Structure | Relation | Surgical Significance |
|---|---|---|
| Recurrent Laryngeal Nerve (RLN) | Runs in the tracheo-oesophageal groove — between the trachea and oesophagus — on its way to the larynx. Passes posterolateral to the thyroid lobe. Enters the larynx posterior to the cricothyroid joint. | Most important nerve to identify and protect during thyroidectomy. Injury → hoarse voice (unilateral) or stridor/aphonia (bilateral). Particularly at risk at Berry’s ligament where it is tethered. |
| External Laryngeal Nerve (ELN) | Branch of the superior laryngeal nerve. Runs with the superior thyroid artery as it approaches the superior pole. Supplies cricothyroid muscle. | Injured when ligating superior thyroid artery too far from the superior pole. Injury → loss of high-pitched voice, inability to shout, pitch fatigue (the “soprano’s nerve”). |
| Parathyroid glands | 4 glands (usually) located on the posterior surface of the thyroid lobes. Superior parathyroids: consistent position at junction of upper and middle thirds, near inferior thyroid artery. Inferior parathyroids: more variable position. | Risk of inadvertent removal or devascularisation during thyroidectomy → post-operative hypocalcaemia |
| Trachea | Immediately posterior to isthmus and lobes. Isthmus overlies rings 2–4. | Tracheomalacia after longstanding goitre; airway emergency post-haematoma |
| Oesophagus | Posterior and slightly left of the trachea | At risk in radical dissection for invasive thyroid cancer; oesophageal injury → mediastinitis |
| Common carotid artery / IJV | Lateral to each lobe within the carotid sheath | Major vascular structures at risk in large goitre or revision surgery |
| Vessel | Origin | Notes |
|---|---|---|
| Superior thyroid artery | First branch of external carotid artery | Runs with the external laryngeal nerve — ligate close to the superior pole to avoid ELN injury |
| Inferior thyroid artery | Thyrocervical trunk (from subclavian artery) | Main blood supply to parathyroids — preservation critical. RLN crosses at this level. |
| Thyroidea ima artery | Brachiocephalic trunk (or aortic arch directly) — present in ~10% | Can be a source of significant intraoperative bleeding if unrecognised; enters at inferior isthmus |
| Superior / middle / inferior thyroid veins | Drain to internal jugular vein; inferior thyroid veins drain to brachiocephalic vein | Multiple venous channels — careful ligation required |
| Lymphatics | Drain to pre-tracheal, paratracheal, and deep cervical nodes | Central compartment (Level VI) is the primary drainage — sentinel node for papillary thyroid cancer |
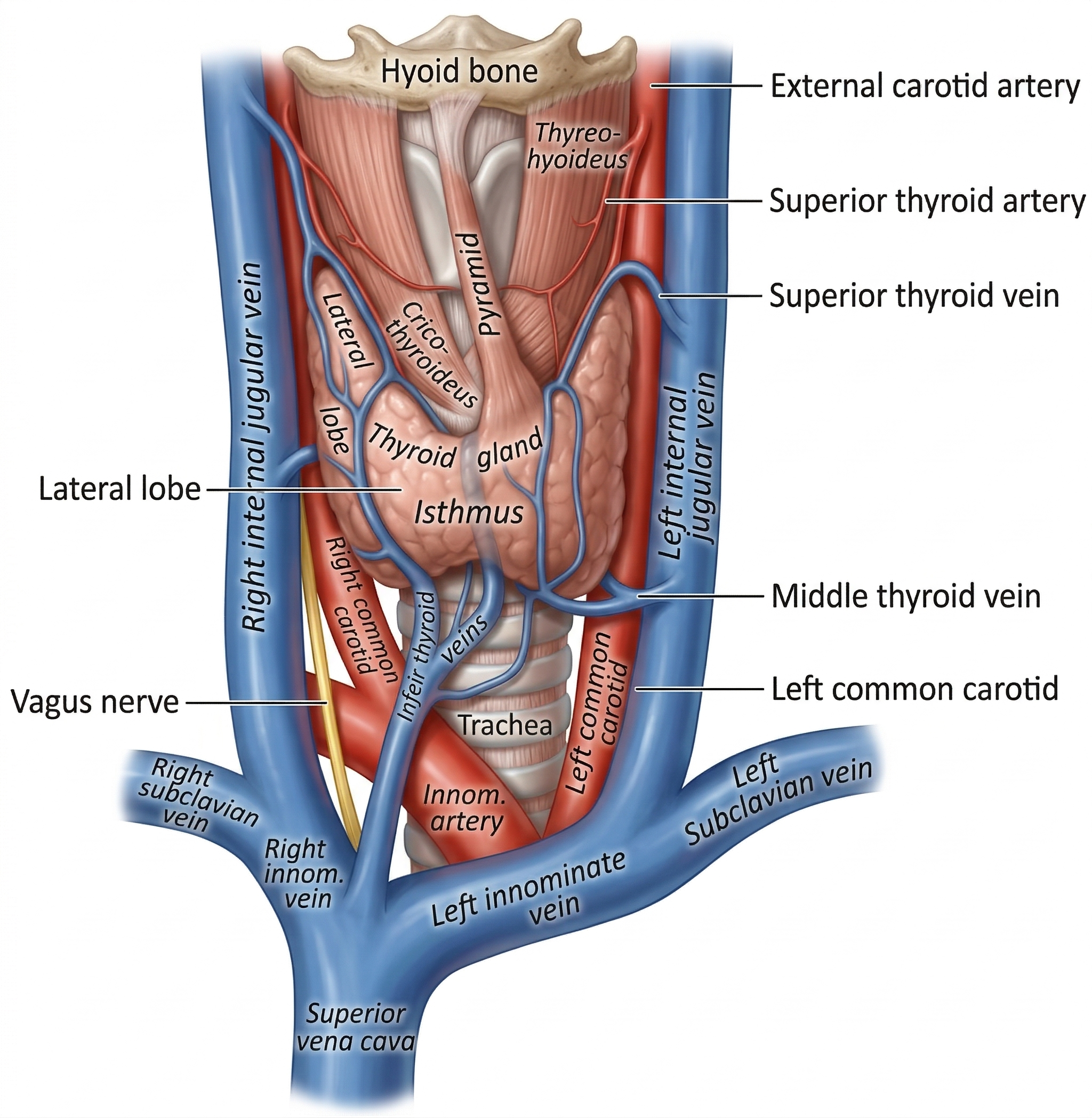
Thyroid Anatomy Diagram
Thyroglossal Cyst — The Classic Embryological Swelling
A thyroglossal cyst forms when the thyroglossal duct fails to fully obliterate after thyroid descent. It presents as a midline neck swelling (or just off midline to the left), typically between the ages of 2–10 years. The pathognomonic clinical sign is upward movement on tongue protrusion — the cyst is tethered to the tongue base via the remaining tract.
Treatment: Sistrunk’s operation — excision of the cyst, the entire thyroglossal tract, and the central portion of the hyoid bone. Removing the hyoid is essential because the tract loops through or around the hyoid body — if the hyoid is not removed, the recurrence rate is ~5–20%; with hyoid excision, it drops to ~3–5%.
Before any operation on a lingual thyroid or midline neck mass presumed to be a thyroglossal cyst, radionuclide scintigraphy must confirm that normal orthotopic thyroid tissue exists. In 1–2% of cases the thyroglossal cyst contains the only functioning thyroid tissue.